Archive \ Volume.11 2020 Issue 4
A Survey of Smoking Habits Among University Students and Its Susceptibility Among Various Diseases
Muhammad Osama Yaseen1*, Arifa Saif 1, Tahir Mehmood Khan1,2, Amal K Suleiman3
1 Institute of Pharmaceutical Sciences, University of Veterinary and Animal Sciences, Lahore, Pakistan. 2 School of Pharmacy, Monash University, Bandar Sunway, Selangor, Malaysia. 3 College of Pharmacy, University of Almaarefa, Riyadh, Kingdom of Saudi Arabia.

Abstract
Purpose: Smoking is the leading cause of death worldwide. Based on recent estimates, there are nearly 1.1 billion smokers worldwide. Smoking habits, perceptions, and beliefs have not been adequately conducted in low-middle income countries (LMICs) like Pakistan, and proper policies have not been made by the government of Pakistan, especially in Health & Education departments. Our study aimed to explore smoking habits among university students and their knowledge, attitude & perception about diseases caused by smoking. Method: A cross-sectional, quantitative study was planned among university students in Pakistan using a structured questionnaire. Statistical methods such as chi-square and sample t-test were performed using SPSS version 21®. Results: Our investigation discovered around 80% non-smokers and 20% of smokers. Anxiety/stress and social influence were the most chosen options with 64.35% and 46.15% votes respectively. 35.4 % of students think they might suffer a smoking-related health issue. The majority of the students professed to have been cautioned in university premises about harms of smoking. 18.96% of people responded that they would continue smoking even knowing the consequences. Rehabilitation centers, pharmacies, and hospitals were the most convenient places for cigarette addicted people to get proper treatment and counseling. Conclusion: The prevalence of smoking among university students was high compared to previous findings and the trend was even higher in female students. The majority of the smokers were reluctant to quit smoking while others would prefer to join rehabilitation centers or seek advice from family and friends.
Keywords: LMICs, Smoking Issues, Health Services Research, Quality of Life

INTRODUCTION
Health is an important factor in life [1]. Smoking is the leading cause of death worldwide [2]. Smoking cessation can reduce the risk of lung cancer [3]. In addition, smoking can also cause excessive melanin deposition in the oral mucosal epithelial layer [4]. Based on the recent estimates, there are nearly 1.1 billion smokers worldwide, of whom 80% resides in low-middle income countries (LMICs). Active smoking led to the death of about 8 million people every year, while 1.2 million deaths are due to passive smoking.[5]
Pakistan is one of 15 countries worldwide with a heavy burden of tobacco-related health problems.[6] Center for Disease Control (CDC) currently estimates that the prevalence of cigarette smoking in Pakistan to be approximately 22.2% in men and 2.1% among women.[7] The annual fatalities that are associated with tobacco use in Pakistan are around 160,100 individuals.[8, 9]
Various studies revealed that the prevalence of smoking is alarmingly high in medical students, doctors, and healthcare professionals, who are supposed to be enforcing initiatives for smoking control and cessation.[10] The physicians and other healthcare professionals are responsible to educate their patients regarding the harms of smoking cigarettes as most people do not give up smoking even if they are counseled properly by the healthcare professionals.[11] Low education was a determinant of cigarette smoking in Pakistan regardless of socio-economic factors. Because people with better education may better understand health information, have a higher locus of control, and may have more information and cognition about the importance of smoking cessation and disease management.[12, 13] A targeted study in Pakistan discovering the prevalence of cigarette smoking, perception, and beliefs of students uncovered high prevalence rates among students, particularly medical students, regardless of awareness about the hazards of smoking.[11]
Investigations related to smoking habits, perceptions and believes have not been adequately conducted in LMICs like Pakistan. There have been very few studies organized in the city of Lahore so far to evaluate the knowledge and attitude about cigarette smoking and still, fewer are those done specifically on university students.[14] Less attention given by the government of Pakistan, Health, and Education departments can be viewed as the absence of comprehensive data on the psychology of smokers and a thorough understanding of the factors motivating people towards smoking.[15] Suitable and long-haul arrangements have not been made and executed by the government and health regulators that could battle with such kind of social issues.
In perspective on all previously mentioned realities, the inspiration driving this investigation is to make a thorough exploratory design with the objectives of covering 1) smoking behavior, 2) perception and knowledge about smoking, 3) awareness about health risks associated with smoking and 4) smoking cessation among university students. Moreover, it will also highlight some coping strategies for the government, health policymakers, and the general public to control the increasing trend of cigarette smoking among university students.
METHODOLOGY:
A cross-sectional descriptive survey was conducted among university students to investigate the perception, level of knowledge, smoking trends, and its association with various diseases. Ethical approval for the study was obtained from the Institutional Review Committee for Biomedical Research, University of Veterinary and Animal Sciences Lahore, Pakistan. The objectives of this study were explained to the respondents before taking their consent. To acquire the trust of participants, information about their national identity card, residents, name, and the mobile number was avoided.
Study location and study duration:
An online survey was conducted among the students from universities and colleges enrolled in Lahore vicinity. The duration of the study was from 1st October 2018 till 31st December 2018. For the evaluation of public knowledge about smoking, a questionnaire was designed which comprised 37 items covering the socio-demographics, smoking behavior and exposure, awareness about harms and risks of smoking, health assessment, and smoking cessation.[16-22] The questionnaire comprised 38 questions out of which six are of socio-demographics and consent while the rest of the questions cover the knowledge, attitudes, and perception of respondents.
Reliability and validity:
A pilot study was conducted on 39 subjects using this questionnaire to further assess its statistical validity. Data analysis is conducted by using Statistical Package for Social Sciences (SPSS) version 21®. The reliability and internal consistency of the test items were confirmed by applying Cronbach’s Alpha test and the results (α=0.71) proved the reliability of the test items.
Sample size:
The sample size of this study was calculated by using a sample size calculator at Raosoft® website [23]. The parameters that need to be considered include the margin of error, confidence level, population size, response distribution, and critical value for the confidence level of this study. In this study, the margin of error and confidence interval was 5% and 95% respectively. The minimum recommended sample size was 377 participants to achieve a 95% confidence level yet 390 respondents were surveyed to make the findings more precise and to give the inhabitants the maximum opportunity to participate in this study.
Data analysis:
The entire questionnaire was assigned a serial number to ensure traceability. The coding of the responses was performed while collected data were processed using SPSS software version 21.0. The data were analyzed by using the appropriate non-parametric statistics such as mean and standard deviation. A Chi-Square test was applied to estimate the association among variables. The difference among the groups was observed using an independent sample t-test. The statistical significance level was 0.05 with a confidence interval of 95%.
RESULTS:
About 487 participants were approached, 390 questionnaires were returned and found complete which complies with the criteria of further analysis with an 80% response rate. 192 (49.23%) of the respondents were female and 197 (50.51%) were male. About 238 (61%) of these respondents were medical students and 152 (39%) were non-medical. 320 (82.1%) of the target population claimed to be non-smokers while 70 (17.9%) were found to be smokers. Summary of demographics is shown in Figure-1. Based on study objectives, the results were divided into five portions namely 1) Smoking behavior and exposure 2) Perception about smoking 3) Awareness about harms and risks of smoking 4) Health assessment 5) Smoking cessation.
These questions on ‘smoking behavior and exposure’ depicted about 312 (80%) non-smokers and 78 (20%) smokers while the majority of cigarette users were regular smokers. The prevalence of smoking among different age groups was 0.76% in 10-13 years, 3.07% in 14-17 years, 10.51% in 18-21years, and 2.05% in 22 years or above. 49 (12.56%) of the current smokers use 1-3 cigarettes per day, 23 (5.89%) use 4-6 cigarettes per day, 10 (2.56%) use 7-9 cigarettes per day and 24 (6.15%) use more than 10 cigarettes per day. 120 (30.76%) people out of the population claimed that their parents or guardians smoke cigarettes. 148 (37.94%) persons out of the total population responded that they have tried to start smoking in the past twelve months. 162 (41.54%) students responded that they were exposed to secondhand smoke in university premises. Further details are given in Table-1.
Upon asking the reason for people to start smoking, anxiety/stress and social influence were the most chosen options with 251 (64.35%) & 180 (46.15%) votes respectively. 58 (74.3%) out of 78 smokers stated that they felt addicted to cigarette smoking while 105 (26.91%) people out of the total population felt they need cigarettes sometimes. 40 (51.2%) of the smokers tried to quit smoking and only a few of them feel irritable or find it hard to concentrate on regular life. Further details are given in Table-2.
242 (62.1%) students believed to have an association of smoking with certain diseases and the statistical analysis proved significant (P=0.07) relation. 138 (35.4 %) students think they might suffer a smoking-related health issue. The majority of students claimed to have been warned in university premises about harms of smoking and 316 (81%) felt that they have adequate knowledge about injurious effects of smoking while results revealed significant value (P=0.041). Watching tobacco promotion ads on television, social media, newspaper, magazines were significantly associated with respondents smoking status (P=0.006). After scoring the whole section and applying the T-test, awareness about the harms of smoking was poor in both genders as the results found out to be non-significant. Further details are given in Table-3.
209 (53.58%) people out of total population claimed to be healthy while the rest suffering from high blood pressure (8.97%), cardiovascular disease (3.07%), diabetes (1.53%), cancer (1.02%), high cholesterol (1.53%), vision problems (22.56%), dental problem (8.97%), depression (16.66%), respiratory problems (6.66%) and others (3.84%) as shown in Figure-2. 163 (41.79%) people do not feel that they are at risk of any disease due to cigarette smoking. 196 (50.25%) students claimed to have respiratory problems due to cigarette smoking. Complete details are given in Table-4.
Results showed a significant relationship (P=0.03) of societal disapproval with smoking cessation. 300 (76.92%) students think that policies should be enforced to ban cigarette smoking, 303 (77.68%) are in favor of sin tax on cigarettes. 153 (64.86%) students wanted to avoid their workplace because of cigarette smokers. Rehabilitation centers, pharmacies, and hospitals were the most convenient places for cigarette addicted people to get proper treatment and counseling as shown in Figure-3. 74 (18.96%) people responded that they’d continue smoking even knowing consequences. Complete details are given in Table-5.
DISCUSSION:
In our study, about 20% of students were smokers and use 1-3 cigarettes per day while the rest were either non-smokers or ex-smokers. In a traditional society like Pakistan, smoking is considered unethical and unacceptable but still, there was a slight increase in smoking trends among female students as compared to previous surveys. This may be accredited to developments in women’s social status e.g. employment, urbanization, and the commercialization of light cigarettes for women. However, the overall prevalence of smoking was higher in males compared to females. Similar findings reported in the 2012 nationwide survey conducted in Pakistan.[12] In developed countries, smoking rates among the female was seen as equivalent to the male as indicated by one investigation.[24] The average age of being a regular smoker was discovered to be 18-21 years in this study. The possible reason could be the social influence because, at this age, students are influenced more by their companions than guardians. A comparable pattern was found in a study claiming that the average age of onset of smoking is 18 years for males and 24 years for females.[25] Another study from Abbottabad, Pakistan revealed that the majority of students start smoking at the age of 15-20 years.[13] However, a study from the USA, Published in Tobacco Induced Diseases 2005, claimed that 55% of students start smoking between the age of 16 and 26 years.[26]
Several factors were found associated with smoking and may have a critical impact on smoking initiation; however, anxiety, stress, and social influence were the fundamental reasons cited by the people. A possible explanation could be that at a certain age students tend to be friends with smokers and would prefer not to be left out of the group of companions merely on the reason for not smoking cigarettes. A study conducted previously at King Edward Medical University, Lahore where students have shown similar trends.[27] Several youths believe that “smoking makes you cool” and that smokers have more friends.[28] There exist many perceptions that relate smoking with the facts that it enhances one’s image, relieves boredom, and helps in easing stress-related issues.[19] Another study suggests that smoking initiation among young adults is stimulated by smoker peers, an attitude of family members, their educational performance, gender, ethnic belonging, socioeconomic status, and psychological distress.[29]
Overall, students were not aware of the harms of smoking (p=0.48); however, non-smokers and the majority of females had enough knowledge about the injurious effects of cigarette smoking. About half of the respondents do not believe to be at risk of any disease associated with smoking while other half believe to be at risk of respiratory problems or might have suffered from respiratory problems due to cigarette smoking. A study conducted in medical students of Agha Khan University, Karachi claimed that most of the students were aware of the harms of both active and passive smoking on health but proper counseling and training were required for smoking cessation and that training should be the part of the medical curriculum.[30]
Our investigative survey from different universities identified some major gaps in students’ practices about cigarette smoking and its cessation. Most smokers are not willing to quit smoking even having enough awareness about its harmful effects. Many of the students preferred their family & friends or to join rehabilitation centers for proper counseling and support in the process of smoking cessation. The worldwide survey of medical students concluded that medical universities of LMICs are deficient in smoking cessation techniques and programs.[31] Lack of systematic approach and adequate training about cigarette smoking and cessation in the university curriculum is of major concern. One reason could be the additional burden of such a curriculum on an already overloaded student. However, we feel that universities should consider the inclusion of additional modules specifically for the training of students about cigarette smoking. Experts working on such programs have reported several obstacles and hurdles in delivering and implementing such programs due to certain reasons but they also have suggested several solutions to overcome such hurdles.[32] The administrative staff of universities and accredited bodies should work in the same direction for the implementation of separate integrated programs about smoking awareness and cessation. Such initiatives have been taken by Indonesia and India by the name “QUIT TOBACCO INTERNATIONAL”.[33] Health education programs should be promoted considering the baseline data of the students’ own beliefs relating to their behaviors about smoking attitudes. Parents should be involved, irrespective of their educational status, in health education projects programmed to highlight their responsibilities towards their children and to encourage them to collaborate in reducing the increased smoking trends in their children. Another model with the name of “mHealth” (Mobile health) implemented in China has been indicated productive in reducing smoking rates with more advantages than conventional labor-derived interventions including its admissibility, flexibility, customizability, adaptability, and versatility to large populations in certain studies.[34] Such models along with tobacco control strategies i.e. ban on public smoking, smoking restriction environment, heavy taxation on tobacco products, awareness advertisements propagating the message of smoking cessation, and sale legislation should be considered by the Government of Pakistan for reducing tobacco consumption. Anti-smoking campaigns should be conducted by the Ministry of Health at the primary and secondary school level to discourage smoking initiation.
Limitations:
The findings of our survey should be transliterated in light of certain limitations we had. Although the population size of our survey was large but due to the investigative nature of our survey on a convenient sample of universities of Lahore, our study only provides a snapshot of universities we surveyed. Investigations of this study may not be generalized to the whole of the universities and the general population of Pakistan. As most of the universities located in urban areas of Pakistan, so this data does not give enough information to students located in rural areas. The only survey-based study was conducted using specifically designed questions from the literature, no psychological techniques were employed to check belief and perceptions of the population. As the data was self-reported, so there is a chance of reporting bias because verification of this self-reported data with a cotinine test was not done since our survey was non-funded. Although participation was not mandatory, and we obtained an acceptable response rate, but selection bias cannot be ruled out.
CONCLUSIONS:
The prevalence of smoking among university students was high compared to previous findings and the trend was even higher in female students. The initiation of smoking was at the age of 18-21 years and possible reasons include anxiety, depression & social influence. Overall awareness level was low in the target population, but certain groups were quite aware of the harms of cigarette smoking. Most of the respondents were free of smoking-related health issues, but some found to be suffered from respiratory problems. The majority of the smokers were reluctant to quit smoking while others would prefer to join rehabilitation centers or seek advice from family and friends. Currently, there are hardly a few studies conducted in the university students of Lahore to evaluate their smoking behavior, perceptions, and beliefs, therefore this study will set a benchmark to lead further research on this issue in Pakistan.
REFERENCES
- Hanawi, S A , Saat, N Z M, Zulkafly, M, Hazlenah, H, Taibukahn, N H, Yoganathan, D et al. Impact of a Healthy Lifestyle on the Psychological Well-being of University Students. Int. J. Pharm. Res. Allied Sci 2020;9(2):1-7
- Kiaee KG, Tabarsy B, Zare M. Effectiveness of problem solving skills and impulse control on the knowledge and attitude of students towards smoking. J. Adv. Pharm. Educ. Res| Apr-Jun. 2019;9(S2):134-138.
- Sholih MG, Perwitasari DA, Hendriani R, Sukandar H, Barliana MI, Suwantika A, Nurmantya I, Diantini A. Risk factors of lung cancer in Indonesia: A qualitative study. J. Adv. Pharm. Educ. Res| Apr-Jun. 2019;9(2):41-45
- AlShoubaki RE, AlZahrani AS. Outcomes of Gingival Depigmentation Among Smokers and Non-Smokers: A Comparative Study. Int. J. Pharm. Res. Allied Sci. 2018 Jan 1;7(1):148-55.
- World Health Organization. Tobacco. 2018; Available from https://www.who.int/en/news-room/fact-sheets/detail/tobacco.
- World Health Organization. Tobacco-Free Initiative (TFI). 2015 November 11; Available from https://www.who.int/tobacco/about/partners/bloomberg/pak/en/.
- Centers for Disease Control and Prevention. Country Reports for All WHO Regions Region, Pakistan. 2014; Available from https://nccd.cdc.gov/GTSSDataSurveyResources/Ancillary/DataReports.aspx?CAID=3.
- Federal Minister for National Health Services Aamer Mehmood Kiani. Tobacco Control Cell, Ministry of National Health Services, Regulations and Coordination, Govt. of Pakistan. 2012; Available from www.tcc.gov.pk/activities.php.
- Tobacco Control Cell, M.O.H.S., Regulations, And Coordination, Government Of Pakistan, Tobacco. 2019; Available from http://www.tcc.gov.pk/activities.php.
- Shah, N., and S. Siddiqui, An overview of smoking practices in Pakistan. Pakistan journal of medical sciences, 2015. 31(2): p. 467.
- Khan, F., et al., Smoking prevalence, knowledge, and attitudes among medical students in Karachi, Pakistan. 2005.
- Gilani, S.I. and D.A. Leon, Prevalence and sociodemographic determinants of tobacco use among adults in Pakistan: findings of a nationwide survey conducted in 20 Population health metrics, 2013. 11(1): p. 16.
- Lodhi, F.S., et al., Inspiration for smoking among medical students of Abbottabad, Pakistan. Journal of Ayub Medical College Abbottabad, 2015. 27(1): p. 178-79.
- Shaikh, B.T., et al., Students, stress, and coping strategies: a case of Pakistani medical school. EDUCATION FOR HEALTH-ABINGDON-CARFAX PUBLISHING LIMITED-, 2004. 17: p. 346-353.
- Nizami, S., et al., Causes of smoking in Pakistan: an analysis of social factors. Journal of the Pakistan Medical Association, 2011. 61(2): p. 198.
- Bobo, F.T., et al., Susceptibility to cigarette smoking and associated factors among high school students in western Ethiopia. BMC research notes, 2018. 11(1): p. 626.
- Kelson, S.R., J.L. Pullella, and A. Otterland, The growing epidemic: a survey of smoking habits and attitudes toward smoking among students in grades 7 through 12 in Toledo and Lucas County (Ohio) public schools-1964 and 1971. American Journal of Public Health, 1975. 65(9): p. 923-938.
- Spillman, D., University students knowledge of cardiovascular disease risk factors. J. Med. Sci, 2003. 3(4): p. 263-273.
- Rozi, S., Z.A. Butt, and S. Akhtar, Correlates of cigarette smoking among male college students in Karachi, Pakistan. BMC Public Health, 2007. 7(1): p. 312.
- Jones, R.M., K.P. Wiseman, and M. Kharitonova, Association between high school students’ cigarette smoking, asthma, and related beliefs: a population-based study. BMC public health, 2016. 16(1): p. 913.
- Omair, A., T. Kazmi, and S. Alam, Smoking prevalence and awareness about tobacco-related diseases among medical students of Ziauddin Medical University. JPMA, 2002. 52(389).
- Taniguchi, C., et al., Development of a new craving index for anticipating quitting smoking in patients who undergo the Japanese smoking cessation therapy. Tobacco Induced Diseases, 2019. 17(December).
- Raosoft. Sample size calculator. [cited 2018; Available from http://www.raosoft.com/samplesize.html.
- Jordan, R.E., et al., Sex, susceptibility to smoking and chronic obstructive pulmonary disease: the effect of different diagnostic criteria. Analysis of the Health Survey for England. Thorax, 2012. 67(7): p. 600.
- Omair, A., T. Kazmi, and S. Alam, Smoking Prevalence and Awareness about ‘tobacco-related Diseases among Medical Students of Ziauddin Medical University. JPMA, 2002. 52(389).
- Von Ah, D., et al., Factors related to cigarette smoking initiation and use among college students. Tobacco induced diseases, 2005. 3(1): p. 27.
- Karamat, A., et al., Cigarette smoking and medical students at King Edward Medical University, Lahore (Pakistan). JPMA. The Journal of the Pakistan Medical Association, 2011. 61(5): p. 509-512.
- Thun, M.J., et al., 50-Year Trends in Smoking-Related Mortality in the United States. New England Journal of Medicine, 2013. 368(4): p. 351-364.
- Tamim, H., et al., Tobacco use by university students, Lebanon, 2001. Addiction, 2003. 98(7): p. 933-939.
- Khan, F.M., et al., Smoking prevalence, knowledge, and attitudes among medical students in Karachi, Pakistan. East Mediterr Health J, 2005. 11(5-6): p. 952-8.
- Richmond, R., et al., Teaching about tobacco in medical schools: a worldwide study. Drug and alcohol review, 2009. 28(5): p. 484-497.
- Chatkin, J. and G. Chatkin, Learning about smoking during medical school: are we still missing opportunities? The International Journal of Tuberculosis and Lung Disease, 2009. 13(4): p. 429-437.
- Nichter, M., et al., Project Quit Tobacco International: laying the groundwork for tobacco cessation in low-and middle-income countries. Asia Pacific Journal of Public Health, 2010. 22(3_suppl): p. 181S-188S.
- Chen+, X., et al., To text or not to text? Acceptability of WeChat and text messaging intervention to promote tobacco control assistance among parents who smoke in rural China. Tobacco Induced Diseases, 2019. 17(December).
|
Table 1: Smoking behavior and exposure |
|||||
|
Question |
Option |
Gender |
|||
|
|
|
Male (n=197) |
Female (n=192) |
Total (%) |
p value |
|
A statement that best describes the responder |
I don’t use cigarettes. |
125 |
186 |
311 (80) |
.000 |
|
I use cigarettes and my parents don't know about it. |
39 |
3 |
42 (10.76) |
||
|
I use cigarettes and my parents don't like it. |
27 |
2 |
29 (7.73) |
||
|
I use cigarettes and my parents don't mind. |
4 |
0 |
4 (1.02) |
||
|
I use cigarettes and my parents don't mind because there are smokers in my family. |
2 |
1 |
3 (0.76) |
||
|
Current non-smoker |
Never smoked |
89 |
178 |
267 (68.71) |
.000 |
|
Former daily smoker |
12 |
2 |
14 (3.58) |
||
|
Former occasional smoker |
37 |
6 |
43 (11.02) |
||
|
Current cigarette smoker |
Daily smoker |
43 |
5 |
48 (12.30) |
.000 |
|
Occasional smoker |
27 |
4 |
31 (7.94) |
||
|
Now occasional smoker, never daily smoker |
7 |
2 |
9 (2.30) |
||
|
Now occasional smoker, formerly daily smoker |
8 |
2 |
10 (2.56) |
||
|
When did you become a regular smoker? |
Never been a regular smoker |
48 |
37 |
85 (21.79) |
.000 |
|
10-13 years old |
2 |
1 |
3 (0.76) |
||
|
14-17 years old |
11 |
1 |
12 (3.07) |
||
|
18-21 years old |
39 |
2 |
41 (10.51) |
||
|
22 years old or older |
7 |
1 |
8 (2.05) |
||
|
On average, how many cigarettes do you smoke per day? |
1-3 |
33 |
16 |
49 (12.56) |
.000 |
|
4-6 |
18 |
5 |
23 (5.89) |
||
|
7-9 |
9 |
1 |
10 (2.56) |
||
|
10 or more |
23 |
1 |
24 (6.15) |
||
|
While you were growing up, how many of your parents or guardians smoked at all? |
None |
132 |
125 |
257 (66.15) |
.804 |
|
One |
37 |
36 |
73 (18.71) |
||
|
More than one |
20 |
27 |
47 (12.05) |
||
|
Not sure |
8 |
4 |
12 (3.07) |
||
|
During the past 12 months, have you tried or thought about smoking? |
Yes |
106 |
42 |
148 (37.94) |
.000 |
|
No |
91 |
150 |
241 (62.05) |
||
|
About how many hours per day, are you exposed to cigarette smoke in University premises? |
Almost none |
95 |
132 |
227 (58.46) |
.006 |
|
Less than one hour |
65 |
42 |
107 (27.43) |
||
|
1-5 hours |
28 |
13 |
41 (10.51) |
||
|
More than 5 hours |
9 |
5 |
14 (3.58) |
||
|
Table 2: Perception of smoking |
|||||
|
Question |
Options |
Gender |
|||
|
|
|
Male (n=197) |
Female (n=192) |
Total (%) |
p value |
|
What do you think are the reasons for people to start smoking? |
Mirroring role models |
45 |
41 |
86 (22.30) |
.164 |
|
Anxiety/Stress |
120 |
131 |
251 (64.35) |
.130 |
|
|
Smoking relaxes the smoker |
70 |
65 |
135 (34.61) |
.722 |
|
|
Way to make friends |
33 |
24 |
57 (14.61) |
.454 |
|
|
Social influence |
83 |
97 |
180 (46.15) |
.164 |
|
|
For the sake of pleasure |
67 |
61 |
128 (33.07) |
.325 |
|
|
Peer influence |
34 |
43 |
77 (19.74) |
.393 |
|
|
Depression |
82 |
86 |
168 (43.07) |
.561 |
|
|
Others |
25 |
13 |
38 (10) |
.002 |
|
|
Have you ever felt like you are addicted to tobacco? |
Yes |
36 |
3 |
39 (10) |
.000 |
|
No |
130 |
171 |
301 (77.43) |
||
|
Maybe |
15 |
4 |
19 (4.87) |
||
|
Have you ever felt like you really needed a cigarette? |
Yes |
58 |
15 |
73 (18.71) |
.000 |
|
No |
121 |
163 |
286 (73.07) |
||
|
Maybe |
18 |
14 |
32 (8.20) |
||
|
Have you ever tried to quit but couldn’t? |
Yes |
33 |
3 |
36 (9.23) |
.000 |
|
No |
76 |
67 |
143 (36.66) |
||
|
Maybe |
3 |
1 |
4 (1.02) |
||
|
When you tried to stop smoking or when you haven’t smoked in a while, did you find it hard to concentrate because you couldn’t smoke? |
Yes |
35 |
3 |
38 (9.74) |
.000 |
|
No |
67 |
41 |
108 (27.69) |
||
|
Maybe |
7 |
0 |
7 (1.79) |
||
|
When you tried to stop smoking or when you haven’t smoked in a while, did you feel more irritable because you couldn’t smoke? |
Yes |
40 |
5 |
45 (11.53) |
.000 |
|
No |
59 |
37 |
96 (24.61) |
||
|
Maybe |
5 |
1 |
6 (1.53) |
||
|
When you tried to stop smoking or when you haven’t smoked in a while, did you feel a strong need or urge to smoke? |
Yes |
39 |
2 |
41 (10.51) |
.000 |
|
No |
54 |
30 |
84 (21.53) |
||
|
Maybe |
12 |
3 |
15 (3.84) |
||
|
Table 1: Awareness about harms and risks of smoking |
|||||
|
Question |
Option |
Gender |
|||
|
|
|
Male (n=197) |
Female (n=192) |
Total (%) |
p value |
|
Do you think you can suffer from a disease caused or aggravated by smoking cigarettes? |
Strongly disagree |
36 |
37 |
73 (18.7) |
.007 |
|
Disagree |
20 |
5 |
25 (6.4) |
||
|
Neutral |
29 |
20 |
49 (12.8) |
||
|
Agree |
25 |
19 |
44 (11.3) |
||
|
Strongly agree |
87 |
111 |
198 (50.8) |
||
|
Do you think you have suffered a health problem as a result of passive smoking (exposure to other people's cigarette smoke) whilst at University premises? |
Strongly disagree |
62 |
45 |
107 (27.7) |
.396 |
|
Disagree |
33 |
25 |
58 (14.9) |
||
|
Neutral |
41 |
45 |
86 (22.1) |
||
|
Agree |
25 |
32 |
57 (14.6) |
||
|
Strongly agree |
36 |
45 |
81 (20.8) |
||
|
When you were in school or college, were you taught about the side effects of smoking such as yellowing of teeth, wrinkles, various diseases, or making smokers smell bad? |
Strongly disagree |
25 |
22 |
47 (12.3) |
.041 |
|
Disagree |
18 |
9 |
27 (6.9) |
||
|
Neutral |
33 |
20 |
53 (13.6) |
||
|
Agree |
38 |
36 |
74 (19.0) |
||
|
Strongly agree |
93 |
105 |
188 (48.2) |
||
|
Do you think you have adequate information about smoking and its risks? |
Strongly disagree |
9 |
6 |
15 (3.8) |
.000 |
|
Disagree |
6 |
3 |
09 (2.6) |
||
|
Neutral |
24 |
25 |
49 (12.6) |
||
|
Agree |
45 |
55 |
100 (25.6) |
||
|
Strongly agree |
113 |
103 |
216 (55.4) |
||
|
When you see cigarette advertisements on television, radio, social media, billboards, posters, newspapers, or magazines, does it incline you towards smoking? |
Strongly disagree |
89 |
124 |
213 (54.9) |
.006 |
|
Disagree |
21 |
19 |
40 (10.3) |
||
|
Neutral |
41 |
25 |
66 (16.9) |
||
|
Agree |
10 |
11 |
21 (5.4) |
||
|
Strongly agree |
36 |
13 |
49 (12.6) |
||
|
Do you think non-medical students of the same age have different perceptions about smoking compared to medical students? |
Strongly disagree |
33 |
29 |
62 (15.9) |
.851 |
|
Disagree |
16 |
19 |
35 (9.0) |
||
|
Neutral |
43 |
44 |
87 (22.6) |
||
|
Agree |
49 |
48 |
97 (24.9) |
||
|
Strongly agree |
56 |
52 |
108 (27.7) |
||
|
Table 2: Health assessment |
|
|||||
|
Question |
Options |
Gender |
|
|||
|
|
|
Male (n-197) |
Female (n=192) |
Total (%) |
p value |
|
|
Are you currently suffering from any of the following conditions? |
High Blood Pressure |
23 |
12 |
35 (8.97) |
.165 |
|
|
Cardiovascular diseases |
8 |
4 |
12 (3.07) |
.520 |
||
|
Diabetes |
3 |
3 |
6 (1.53) |
.992 |
||
|
Cancer |
3 |
1 |
4 (1.02) |
.615 |
||
|
High Cholesterol |
3 |
3 |
6 (1.53) |
.992 |
||
|
Vision Problems |
31 |
57 |
88 (22.56) |
.004 |
||
|
Dental Problems |
14 |
21 |
35 (8.97) |
.397 |
||
|
Depression |
23 |
42 |
65 (16.66) |
.024 |
||
|
Respiratory problems |
13 |
13 |
26 (6.66) |
.963 |
||
|
Any other disease |
4 |
11 |
15 (3.84) |
.162 |
||
|
None |
116 |
92 |
208(53.58) |
.062 |
||
|
Being a smoker or secondary smoker (non-smoker), do you feel you are at a risk of? |
High blood pressure |
36 |
23 |
59 (15.12) |
.204 |
|
|
Cardiovascular diseases |
38 |
25 |
63 (16.15) |
.222 |
||
|
Diabetes |
8 |
10 |
18 (4.61) |
.844 |
||
|
Cancer |
40 |
38 |
78 (20) |
.875 |
||
|
High cholesterol |
8 |
5 |
13 (3.33) |
.714 |
||
|
Vision Problems |
12 |
14 |
26 (6.66) |
.862 |
||
|
Dental Problems |
20 |
17 |
37 (9.48) |
.862 |
||
|
Depression |
21 |
20 |
41 (10.51) |
.940 |
||
|
Respiratory Problems |
65 |
76 |
141(36.41) |
.167 |
||
|
Any other Disease |
11 |
12 |
23 (5.89) |
.932 |
||
|
None |
90 |
73 |
163(41.79) |
.216 |
||
|
Has cigarette smoke ever triggered breathing problems or cough related symptoms in you? |
Yes |
80 |
115 |
195(50.25) |
.003 |
|
|
No |
77 |
46 |
123(31.53) |
|||
|
Uncertain |
40 |
31 |
71 (18.20) |
|||
|
Table 3: Smoking cessation |
|||||
|
Question |
Options |
Gender |
|||
|
|
|
Male (n=197) |
Female (n=192) |
Total (%) |
p value |
|
Do you think people in your neighborhood or community view cigarette smoking among adults as acceptable? |
Strongly disagree |
52 |
51 |
103 (26.41) |
.619 |
|
Disagree |
19 |
17 |
36 (9.23) |
||
|
Neutral |
49 |
41 |
90 (23.07) |
||
|
Agree |
45 |
42 |
87 (22.30) |
||
|
Strongly agree |
32 |
41 |
73 (18.97) |
||
|
Can societal disapproval of smoking lead to smoking cessation? |
Strongly disagree |
20 |
15 |
35 (9.23) |
.031 |
|
Disagree |
22 |
17 |
39 (10) |
||
|
Neutral |
66 |
55 |
121 (31.02) |
||
|
Agree |
44 |
38 |
82 (21.02) |
||
|
Strongly agree |
45 |
67 |
112 (28.71) |
||
|
Should policies that don't allow cigarette smoking in indoor or outdoor public places be strictly enforced? |
Strongly disagree |
10 |
11 |
21 (5.38) |
.401 |
|
Disagree |
14 |
4 |
18 (4.61) |
||
|
Neutral |
29 |
22 |
51 (13.07) |
||
|
Agree |
31 |
27 |
58 (14.87) |
||
|
Strongly agree |
113 |
128 |
241 (62.05) |
||
|
Would you be in favor of an increase in the tax on a pack of cigarettes if the money is used to improve the public's health? |
Strongly disagree |
30 |
5 |
35 (8.97) |
.000 |
|
Disagree |
14 |
3 |
17 (4.35) |
||
|
Neutral |
18 |
16 |
34 (8.97) |
||
|
Agree |
22 |
19 |
41 (10.51) |
||
|
Strongly agree |
113 |
149 |
262 (67.17) |
||
|
Have you ever wanted to move away from where you are working because of other people's cigarette smoke? |
Strongly disagree |
30 |
15 |
45 (11.53) |
.003 |
|
Disagree |
20 |
11 |
31 (7.94) |
||
|
Neutral |
40 |
21 |
61 (15.64) |
||
|
Agree |
29 |
25 |
54 (13.84) |
||
|
Strongly agree |
78 |
120 |
198 (51.02) |
||
|
Would you still continue smoking or smoke in future knowing all the consequences you might have to bear because of smoking? |
Strongly disagree |
69 |
132 |
201 (51.79) |
.000 |
|
Disagree |
26 |
7 |
33 (8.46) |
||
|
Neutral |
53 |
28 |
81 (20.76) |
||
|
Agree |
20 |
6 |
26 (6.66) |
||
|
Strongly agree |
29 |
19 |
48 (12.30) |
||
|
From where you think it's convenient to get help regarding smoking cessation? |
Rehabilitation centers |
99 |
132 |
231 (59.23) |
.000 |
|
Hospitals |
56 |
44 |
100 (25.64) |
.388 |
|
|
Pharmacies |
31 |
48 |
79 (20.51) |
.011 |
|
|
Clinics |
39 |
33 |
72 (18.46) |
.716 |
|
|
Helplines |
24 |
27 |
51 (13.07) |
.797 |
|
|
Specified societies of university |
71 |
70 |
141 (36.15) |
.750 |
|
|
Family/Friends |
134 |
125 |
259 (66.66) |
.646 |
|
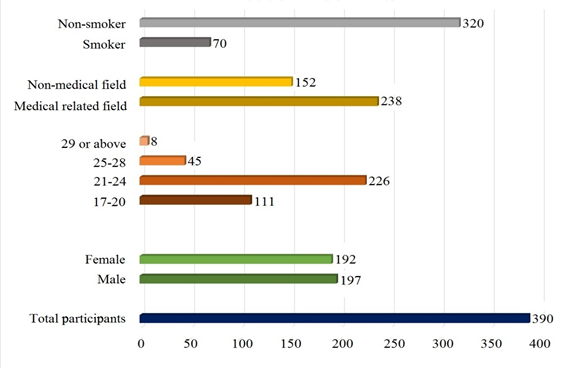
Figure 1: Demographic information of respondents
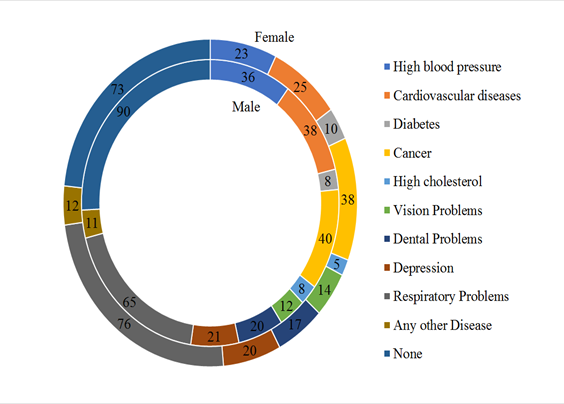
Figure 2: Percentage of disease-risk population
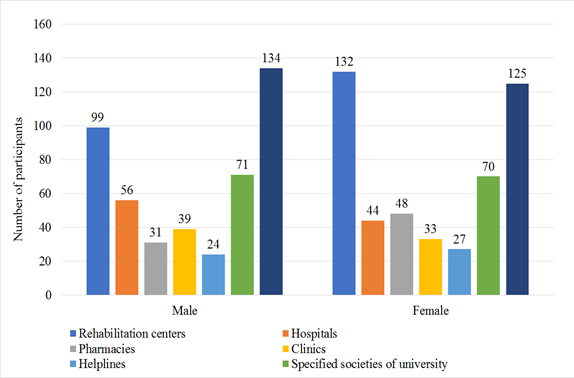
Figure 3: Public opinion about smoking cessation
