Archive \ Volume.14 2023 Issue 2
Impact of Ayush Alternative Medicine Interventions in the COVID-19 Pandemic
Rajorshi Sen Gupta1, Sandip Roy1*, Rajesh Bose1, Palash Mandal2
1Department of Computational Science, Brainware University, Barasat, India. 2Nanobiology and Phytotherapy Laboratory, Department of Botany, University of North Bengal, Siliguri, India.
Abstract
The five Indian systems of alternative and complementary medicine (Ayurveda, Yoga, Naturopathy, Unani, Siddha, and Homeopathy) are frequently used to treat "COVID-19" throughout the country (referred to simply as "AYUSH"). At the outset of the pandemic, "The Ministry of AYUSH" (the governing authority of the Indian system of medicine) issued recommendations for the use of particular herbs and acts to improve immunity, based on the advice of an advisory council of "AYUSH" doctors and scant evidence. Some of these suggestions involved using traditional herbs and practices, which have been used for centuries and are effective in treating a wide range of conditions, including fever, sore throat, and breathing difficulties, as well as acting as a non-specific leniency enhancer thanks to their anti-viral, anti-bacterial, and anti-microbial properties. A number of the formulations recommended here—including AYUSH 64, Chyawanprash, Guduchi Ghanavati, Arsenic Album, Kabasur Kudineer, and Nilavembu Kudineer—have been the subject of scientific research into their putative prophylactic or therapeutic benefits.
Keywords: Coronavirus, Cytopathic, Meta-analysis, Disease
INTRODUCTION
Because there is now no effective pharmaceutical available, people are increasingly looking to alternative remedies for help. Multiple nations are actively researching "COVID-19" using ACMs. To help in the prevention and treatment of "COVID-19", many countries have established recommendations on the use of traditional medicines. Many programs have been started to back up the studies being done in “TICAM (Traditional, Integrative, Complementary, and Alternative Medicine)” to better incorporate the existing traditional knowledge [1]. Commonly utilized in India for the treatment of "COVID-19" are the five alternative and complementary treatments known as “Ayurveda, Yoga, Naturopathy, Unani, Siddha, and Homeopathy” (referred to simply as "AYUSH") [2]. “The Ministry of AYUSH” (the governing authority of the Indian system of medicine) released guidance at the start of the epidemic, recommending the use of certain herbs and actions to boost immunity, based on the recommendation of an advisory group of "AYUSH" specialists and rudimentary evidence. These recommendations included the use of traditional herbs and methods, which have been around for decades and be effective in treating a variety of conditions such as fever, sore throat, and breathing difficulties as well as acting as a non-specific leniency enhancer thanks to their anti-viral, anti-bacterial, as well as anti-microbial characteristics. Some of the suggested formulas have been studied scientifically for their potential preventative or therapeutic effects; they are “AYUSH 64, Chyawanprash, Guduchi Ghanavati, Arsenic Album, Kabasur Kudineer, and Nilavembu Kudineer” [3]. Several randomized controlled studies of "AYUSH" therapies have either been published or are underway. These research results need to be thoroughly reviewed and described using evidence syntheses to ascertain the quality of the evidence.
The time has come for "AYUSH" health officials to review and update the "COVID-19" recommendations using an evidence-based approach that takes into account the most recent and best available research. The purpose of this review and meta-analysis is to determine whether or not "AYUSH" systems of medicine, which are part of India's traditional medical practice, are successful in lowering the prevalence, severity, and length of "COVID-19" [4]. The disadvantage of traditional systematic reviews is that they only give an overview of the pertinent evidence at a single point in time; live systematic reviews overcome this problem by providing regular updates. Suggestions and clinical guidelines can benefit from periodic updates, and a complete and up-to-date evaluation of the evidence can be provided by a live systematic review.
MATERIALS AND METHODS
The complexity Significant morbidity and death have resulted from the worldwide spread of “serious acute respiratory disorder coronavirus 2 (SARS-CoV-2)”, producing coronavirus infection 2019 (COVID-19) [1]. Through the end of February 2022, nearly 6 million deaths were attributed to “COVID-19”, which had caused over 428 million cases worldwide. Out of a total of 42 million positive cases, almost 5 lakh people died in India. On other continents, researchers have discovered a mutation in the form of “SARS-CoV-2” that may be transmitted to humans, causing a greater public health crisis [4]. The development of vaccines and treatments for this new coronavirus is a top priority for scientists throughout the world. The numbers show that even with the best efforts of many people in the medical and governmental fields, the number of instances keeps rising. “Remdesivir, Dexamethasone, and a few monoclonal antibodies” are recommended for in-hospital use, although their effectiveness is low. Azithromycin and hydroxychloroquine were repurposed as “COVID-19” treatments to find a solution more quickly, but the results were disappointing. Currently, there are no effective pre-exposure chemoprophylactic treatments available.
Quality or Risk of Bias Assessment of AYUSH Intervention
Separately, two reviewers evaluated each study because of its potential for bias. “Randomized controlled trials” (RCTs) were evaluated utilizing “Risk of Bias in Randomized Research of Interventions” (ROBINS-I), whereas non-randomized research was evaluated using the "Revised Cochrane" method for "assessing the risk of bias RoB-2". Research Studies (NRIs) to evaluate studies based on their outcomes [5]. Domains for such "RoB-2 tool12" included puzzling, bias throughout the selection of participants, as well as bias mostly in the categorization of intervention strategies, while those for the "ROBINS-I tool13" included confounding, bias in the quantification of the results, as well as bias emerging as from permutation process. Studies were classified as having either i) minimal risk of bias, ii) some concerns, or iii) a significant risk of bias within each of these areas. Overall, there was little to no prejudice because that was the case in all areas. Studies were deemed high risk whenever at minimum one domain was deemed toward being large probability, and yet when various samples were deemed to be some worry, the total bias threat was graded as being some kind of concern. When necessary, a third reviewer was brought in to mediate disagreements between the two groups of reviewers.
|
|
|
Figure 1. Critical analysis of CTRI (Source: https://ars.els-cdn.com/content/image/1-s2.0-S0975947620301030-gr1.jpg) |

The New Indication for "Covid-19"
The suggestions of such an Interdisciplinary "AYUSH R & D Task Force" established by the Ministry of AYUSH, combined with current quality requirements, proofs on diagnostic including pre-clinical security, as well as evidence on effectiveness in Influenza-like disease, led to the repurposing of "AYUSH-64 for"covid-19" ". The fresh indication is established based on the drug's anti-viral as well as naturally resistant action, along with the evidence gleaned from the molecular docking research mentioned above. According to the Indian Clinical Trials Registry, seven clinical trials on AYUSH-64 have been conducted in asymptomatic with mild-to-moderate "COVID-19" patients at reputable medical facilities in India. Within those clinical trials, AYUSH-64 has been used both as a stand-alone therapy for asymptomatic with mild instances of"covid-19" as well as an addition to normal care for "mild and moderate" symptoms of"covid-19" [6]. The results of these trials showed that adding "AYUSH-64" to normal therapy sped up recovery time without increasing the risk of the disease progressing to a crucial moment. In addition, the AYUSH-64 supplement group had a shorter median time to a false RT-PCR result for"covid-19". There was also a rise in QoL (Quality of Life) indicators. The results showed that AYUSH-64 was effective and had good safety profiles.
The National COVID care regimen based on "Ayurveda and Yoga" now includes "AYUSH-64 for asymptomatic and mild cases of"covid-19" " based on the results developed via clinical and experimental research. During the second"covid-19" epidemic in the nation, the Ministry of AYUSH produced "Guidelines for Ayurveda Practitioners for"covid-19" Patients in Home Isolation," which includes AYUSH-64. To ease pressure on hospitals, the "Ministry of AYUSH" has also begun a widespread effort to provide AYUSH-64 to people living with"covid-19” who became asymptomatic or only have moderate to mild symptoms at home. This review aims to provide a scientific explanation of the basic treatment strategy of AYUSH-64 within the context of"covid-19", specifically in its different clinical and pathologic phases.
|
|
|
Figure 2. Ayurvedic parameters of Ayush 64 (Source: https://ars.els-cdn.com/content/image/1-s2.0-S0975947620300255-gr3.jpg, 2022) |

Infection and Transmission of "Covid-19"
The "SARS-CoV-2" virus is airborne and travels from infected person to person through their coughs and sneezes. The incubation time is usually between five and six days but can last anywhere from one to fourteen days in total. Although the patient could often stay for around two weeks, the risk of transmission is at its highest during the first week or so. Some people may be infected for several weeks without showing any symptoms, and these people are regarded as long-term spreaders [7]. Many people with"covid-19” become infected before they show any symptoms, while many others are afflicted and show no signs of illness. Hence, monitoring these mutations is crucial for pandemic control. Even during the second"covid-19" epidemic, about 80% of people had no symptoms or showed only mild ones, 15% showed moderate to serious complications and required oxygen assistance, and 5% showed the imminent emergency necessity for mechanical breathing. Hospitalized patient deaths averaged over 11% globally, however, it amounted to less than 1.1% throughout India.
|
|
|
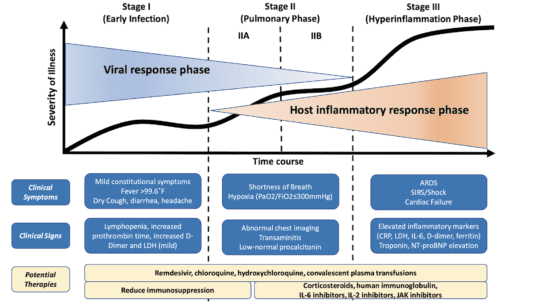
Figure 3. Clinical stage of"covid-19" (Source: https://rebelem.com/wp-content/uploads/2020/03/COVID-19-Classification-539x303.png)
|

Analysis of such viral dynamics shows that the clinical result of"covid-19" remains the same regardless of such viral load. In moderate cases, the infection clears on its own during the early stages, but in serious forms, viral shedding persists for a longer period. Inconsistent results have been found in the investigations conducted thus far on the dynamics of parasitic infections. The patient can continue shedding this virus long after their symptoms have subsided. In those who make it, the average time it takes for the virus to transmit is approximately 20 days. Long-term consequences of"covid-19” have been documented in some people who initially presented with just modest signs of the illness. An in-depth knowledge of such molecular mechanisms involved in"covid-19” pathogenesis seems required for the design of efficient treatments and preventative strategies. Recent research into the causes of"covid-19” has shown a pathogenesis pathway with three clinically different but potentially overlapping stages. Phases of viral replication or primary infection, the pulmonary phase, the "pro-inflammatory phase", as well as the "pro-thrombotic phase" are depicted.
Immune Response and Clinical Features of "Covid-19"
Symptom presentation varies from person to person as a consequence of immune system differences. Positive "RT-PCR" but no symptoms indicate an asymptomatic case of"covid-19"; low to high disease; positive alongside clinical signs; severe overall critical disease (positive with a high degree of manifestations). Healthcare workers with"covid-19” typically experience a rise in C- reactive protein (>20 mg/dl) as well as a wide range of other symptoms, including "fever (83-98%), fatigue (70%), dry cough (82%), headache (34%), dyspnea (50%), sore throat (14%), rhinorrhea (7%), loss of smell and loss of taste (7%), diarrhea (20%), vomiting (14%) and weakness (70%)". Compared to moderate instances (CRP 18 mg/dl), severe and critical cases have higher CRP concentrations (>40 mg/dl and >100 mg/dl, respectively) [8]. Those with the most severe cases also have an elevated absolute" lymphocyte" count (100 cells/l). For moderate"covid-19", look for a pulmonary function of over 30 breaths per minute and oxygen saturation (SpO2) of less than 90% [9]. Some people with"covid-19" develop the last level of the disease, which is characterized by acute inflammation seen in the form of a cytokine storm including extensive platelet aggregation that ultimately results in multi-organ dysfunction. Over the first several days after infection, a person experiences the "replication stage", followed by the "adaptive immunity stage". In the replication phase, the virus causes moderate flu-like symptoms according to its direct "cytopathic" action (structural alterations in host cells). During the "adaptive immunity phase", the viral load decreases as the immune system assumes over, but during the "inflammatory phase, a "cytokine storm" might cause tissue damage and a worsening clinical situation.
Mitigation of Psychological Impact of"Covid-19"
Ten "Yoga & Naturopathy" studies and the first Ayurvedic study looked at reducing"covid-19" -related psychological stress as well as its accompanying symptoms, which include sadness, anxiety, and sleeplessness. One out of ten "Yoga and Naturopathy" studies was found to be single-armed, while the other nine were either double- or single-blind [10]. Four randomized controlled trials compared "conventional care" (CC) with and without intervention. The remaining five trials all used placebos, no treatment, relaxation techniques, or counseling as comparison groups. Six studies focused on those at high risk, whereas the seventh solely included healthy volunteers. Three more trials were conducted, one of which included asymptomatic participants and patients with overall minor to moderate illness, and the other two included patients who had mild to moderate disease. Six trials did not report the duration of treatment [9]. The remaining dominant research reported a length of seven days, another reported fifteen, and two others reported more than thirty. Only two studies had a total study period of fewer than six months, whereas five lasted between 3 and 6 months, as well as three lasted for a full year. Study after study has found that measuring psychological states like depression, anxiety, stress, sleeplessness, etc., as main findings to be quite useful. Stress scale and serum cortisol level were both included as the outcome measure of one research. The sole Ayurvedic study regarding stress reduction used a double-blind design [10]. The Brahmi (Bacopa monnieri) group received therapy, whereas the control group received nothing. In this study, researchers considered 201 healthy participants for two months. There was no mention of how long therapy would last.
|
|
|
Figure 4. Sustainability of Public health care (Source: https://www.mdpi.com/sustainability/sustainability-13-03415/article_deploy/html/images/sustainability-13-03415-g001-550.jpg) |

Clinical Improvement: Add-on AYUSH Interventions vs. Standard Care
The results of two randomized controlled trials (n=81) showed clinical improvement as an outcome. Additional AYUSH interventions were associated with a slightly higher percentage of"covid-19" patients reporting clinical improvement compared to standard care, but this difference was not statistically significant [rate ratio [RR] 1.24 (95% confidence interval [CI]: 0.61 to 2.53; risk difference [RD] 132 for every 1,000 (from 215 lesser to 841 more). Because of the many treatments, there was a large amount of heterogeneity (I2=81%) [11]. As a result of considerable bias, heterogeneity, and imprecision across both studies, the level of evidential confidence is low at best.
|
|
|
Figure 5. Chart of clinical improvement [9] |

Viral Clearance: Add-on AYUSH Interventions vs. Standard Care
Viral clearance was determined using polymerase chain reaction cutoff points in three randomized controlled trials (n=163) of supplementary AYUSH interventions [12]. The proportion of patients who received either AYUSH supplements or conventional therapy did not change significantly between the two groups [RR 1.19 (95% CI: 0.59 to 2.42)] or at 99 cases per 1,000 (from 214 reduced to 741 more). There is no substantial heterogeneity (I2=82%) between the trials' findings when it comes to the therapies they tested. Low levels of evidential reliability were seen, together with high levels of imprecision and large variability.
|
|
|
Figure 6. Viral clearance graph (Add-on AYUSH intervention) [8] |

Viral Clearance: Standalone AYUSH Interventions vs. Standard Care
Virus eradication was reported in three randomized controlled trials of AYUSH therapies RCTs (283). With intermediate certainty, there was an increase in the number of patients reporting a negative RT-PCR in the group that received solitary AYUSH therapies [RR 1.32 (95% 16 CI: 1.20 to 1.47); risk difference 228 more for each 1,000 (from 143 more to 335 more)] [13]. Since there was no discrepancy across results (I2=0%), researchers may conclude that the research was homogenous. The high potential for bias reduced the level of assurance to that moderate. Pictured: (Figure 7a) the results of a single NRSI suggest that AYUSH on its alone may improve viral elimination in"covid-19” individuals [RR 6.22 (95% CI: 3.28 to 11.77)], which is consistent with meta-analyzed evidence from randomized controlled trials.
|
|
|
a) |
|
|
|
b) |
|
Figure 7. a) Viral Clearance (Standalone AYUSH intervention) [10], b) Forest Plot of AZD1222 and BBIBP-CorV vaccine. Covishield vs Sniopharm vaccine of China can be depicted from this Forest plot. |


Two tablets of AYUSH-64 (500 mg each) were recommended for asymptomatic patients with COVID-19 to take twice daily with warm water after meals, and for symptomatic patients (mild/moderate), two tablets of AYUSH-64 (500 mg each) were recommended to take thrice daily. Based on the local healthcare provider's assessment of the severity of the condition, the MoHFW recommended using the intervention in addition to the conventional care guidelines for treating COVID-19. The Indian Medicines Pharmaceutical Corporation Limited, a GMP-certified producer, supplied the AYUSH-64 used in this study, therefore its quality was guaranteed (IMPCL). AYUSH-64 is a combination of many herbs, including: “Saptaparna (Alstoniascholaris R. Br.), Katuki (PicrorhizakurroaRoyle ex. Benth.), Kiratatikta (SwertiachirataPexbex. Karst.)”, and Kuberaksha (Berberisaristata DC. It is the well-validated ideas and practices of the AYUSH systems that are the focus of this research, as they may be utilized to better comprehend, diagnose, and develop therapies for emerging disorders such as COVID-19. Clinical symptoms (cough, fever, respiratory distress, etc.) related to COVID-19 can be managed using a wide variety of treatments (medicines, procedures, nutrition, no pharmacological regimens) provided by these systems. When it comes to treating this cluster of symptoms, AYUSH practitioners turn to a wide variety of tried-and-true medicinal options. The researcher is responsible for justifying the intervention chosen among the many that exist in the AYUSH literature. Furthermore, the Investigator should give evidence of the benefits and harms of the therapies included in the trial, and should propose a credible explanation for how the interventions could operate.
RESULTS AND DISCUSSION
There was one randomized controlled trial (RCT) that suggested a possible reduction in the incidence of"covid-19" infection due to a standalone AYUSH intervention, but the result was not statistically significant [rate ratio [RR] 0.48 (95% confidence interval [CI]: 0.09 to 2.58); 22 some less for every 1,000 (from 38 lesser to 67 more)]. The results of one NRSI 22 study suggested that a single AYUSH intervention may have had a negligible or nonexistent impact on the rate of"covid-19” infection [rate ratio [RR] 0.79 (95% confidence interval [CI] 0.44 to 1.41], or 1 fewer cases per 1,000 [from 2 fewer to 1 more] [14]. Due to the substantial possibility of prejudice and imprecision in both investigations, confidence in the data was poor.
Researchers were unable to conduct a subgroup analysis because researchers lacked the raw data that would have been needed to do so. Researchers examined the robustness of meta-analytic results by first varying the statistical model used (control variables vs. random effect) and then by secondly switching the influence of measurements (“RR by OR by RD or MD by SMD”). When researchers switched the equation from conditional variance to a fixed-effect model in the sensitivity analysis, researchers saw the same patterns across all four outcomes. When effect measurements (RR/MD) were swapped out for anything else, the results' significance remained unaffected. Analysis of sensitivity data revealed that the results were stable and repeatable.
Up to April 2, 2021, this ongoing literature review and meta-analysis provide a comprehensive overview of the evidence for AYUSH therapies with COVID-19. There were a total of 12 randomized controlled studies, with six focusing on AYUSH treatments used alone and the other six on AYUSH treatments used in conjunction with conventional medicine. As an example, only Ayurveda and Siddha research publications may be found in AYUSH aggregators. The use of alternative medical practices like “Yoga, naturopathy, Unani, or homeopathy” was not recorded in any of the research. The AYUSH-64 Guduchi Ghanavati, Chyawanprash, and five other regimens were employed as interventions in “Ayurveda”, whereas in “Siddha”, a single regimen including mostly Kabasura Kudineer was utilized [15]. The Ayurvedic and Siddha medications were included in one treatment plan. The lack of mortality recorded or the low number of events reported on oxygen therapy/ventilator usage in studies may be because all available information comes from mild to moderate patients. So far, investigations on COVID-19 patients have produced scant data concerning the negative consequences of most therapies. Since there was a substantial possibility of bias and/or imprecision, the evidence was of moderate to low quality. Unmasking, a lack of allocation concealment, improper reporting of data, and the incorporation of NRSI all contributed to a potentially high risk of bias in the studies included; nevertheless, NRSIs were synthesized independently. A meta-analysis found that AYUSH interventions, both as an adjunct and on their own, may speed up the rate at which symptoms improve and the virus is cleared from the body. Although integrated usage may be convenient, there is no evidence to suggest it improves therapeutic outcomes in terms of virus clearance or patient health. When used as preventative measures, AYUSH therapies may lessen the spread of COVID-19.
Comparison between Multiple COVID-19 Vaccines
As observed from the forest plot, it can be stated that the sensitivity of Sniopharm is more than Covishield. This means that the vaccine is also more effective against small viral loads present in the human body. This sensitivity plays a major role in increasing the production of antibodies for fighting viral antigens present in the human body. On the other hand, it can be said that the Indian-produced COVISHIELD has less sensitivity than the China counterpart. Therefore, it is not specifically effective at small viral loads as Sinopharm is. On January 28, 2021, COVID-19 vaccinations were introduced to Morocco, and anyone aged 18 and above was advised to be vaccinated. Five different COVID-19 vaccines are currently in use in Morocco. These include an inactivated virus vaccine (Beijing CNBG's BBIBP-CorV), two viruses vectored vaccines (AstraZeneca's Vaxzevria and Gamaleya's Gam-COVID-Vac), a messenger RNA vaccine (Pfizer-Comirnaty), BioNTech's and a modified virus vector vaccine (Janssen's).
Conclusions from the phase III clinical trials of Sinopharm's BBIBP-CorV were consistent with their expected efficacy [8].
In the real world, two doses of BBIBP-CorV substantially reduced the risk of severe or critical hospitalization due to COVID-19 in individuals of working age and had a modest impact on the elderly. Although a small percentage of participants got booster doses, this was linked with full protection at any age.
CONCLUSION
As the first study to focus on AYUSH therapies in"covid-19", this updated systematic literature review will provide a comprehensive summary of such Indian Traditional Medical System's arsenal against the virus. It will help doctors, policymakers, as well as others make educated choices about the role of AYUSH therapies in the treatment of"covid-19". Variations in the "Population, Intervention, Comparator, and Outcome (PICO)" of valid evidence as well as the quality of such methodology across them will have the greatest impact on the accuracy and credibility of the results. We intend to incorporate pre-prints because of the significance of the data they provide and the likelihood that much research will appear initially in preprint archives. Since favorable result studies seem to be more probable to be published than negative ones, publication bias is possible; however, incorporating pre-prints may mitigate this effect.
ACKNOWLEDGMENTS: None
CONFLICT OF INTEREST: None
FINANCIAL SUPPORT: None
ETHICS STATEMENT: None

{kind=link}