Archive \ Volume.11 2020 Issue 1
Relation between Coronary Arterial Remodeling and Characteristics of Atherosclerotic Plaque Determined
by Intravascular Ultrasound
Sy Van Hoang 1,2*, Kha Minh Nguyen 1, Hung Phi Truong 1,2, Luan Tri Mai 3, Hai Phuong Nguyen Tran 3
1 Internal Medicine Department, Faculty of Medicine, University of Medicine and Pharmacy at Ho Chi Minh City, Vietnam. 2 Cardiovascular Department, Cho Ray Hospital, Ho Chi Minh City, Vietnam. 3 Interventional Cardiology Department, Cho Ray Hospital, Ho Chi Minh City, Vietnam.

Abstract
Background: Coronary arterial remodeling, which is the change in vessel size due to the presence of atherosclerotic lesions, is associated with plaque characteristics and clinical presentation. However, most studies have included patients with distinct levels of coronary artery stenosis. Objectives: The aim of this study was to assess coronary arterial remodeling and its relationship with the plaque features of coronary atherosclerosis determined by intravascular ultrasound (IVUS) in patients with moderate coronary artery stenosis. Methods: In total, 215 patients with lesions with moderate stenosis underwent UVIS imaging. Measurements included minimal lumen area, total artery area, average reference artery area, plaque area, plaque burden, eccentricity index, and remodeling index (RI). RI>1.0 was defined as positive remodeling and RI≤1.0 as negative remodeling. Results: In total, 88 patients had positive remodeling and 127 had negative remodeling. The two types of remodeling did not differ in terms of patient characteristics and risk factors (p>0.05). The acute coronary syndrome was more common in positive remodeling than in negative remodeling (47.7% vs. 8.7%; OR=9.63; 95%CI: 4.56–20.31; p<0.001). The positive and negative remodeling groups differed significantly in the level of stenosis (43.29±18.80% vs. 50.21±14.31%; p=0.003), plaque area (9.40±3.93 mm2 vs. 7.58±3.29 mm2; p<0.001) and plaque burden (68.95±10.38% vs. 63.76±10.27%; p<0.001), but not in lumen area or eccentricity index (p>0.05). Conclusion: Positive vascular remodeling was more prevalent in acute coronary syndrome than instable angina and had a larger plaque area and a higher plaque burden than negative remodeling. Nevertheless, the stenosis level was still lower with positive remodeling.
Keywords: Coronary arterial remodeling, Plaque characteristic, Intravascular ultrasound

INTRODUCTION
Atherosclerosis could be a common sickness that is seriously harmful to human health. [1] It is a disease in which plaque – consisting of fat, cholesterol, calcium, and other substances found in the blood – builds up inside arteries. [2, 3] Atherosclerosis is presently viewed as the main underlying reason for myocardial infarction and causes millions of deaths around the world. Understanding this disease in terms of the differences in its plaque features may improve the treatment and prevention of cardiovascular disease.
In 1987, Glagov et al. [4] reported that human coronary arteries undergo compensatory enlargement in the presence of atherosclerosis – a phenomenon subsequently designated coronary arterial remodeling or Glagov’s phenomenon. Coronary arterial remodeling that maintains the size of the coronary artery at the early stages of atherosclerosis is known as positive remodeling.
However, numerous intravascular ultrasound (IVUS) studies have demonstrated that vasoconstriction can lead to a local shrinkage of vessel size, rather than dilation. This condition is defined as negative remodeling. [5, 6]
IVUS is an established imaging technology that can be useful for evaluating coronary arterial structure, geometry, and vascular remodeling. [7, 8] An increasing number of studies have shown an association between vascular remodeling and clinical aspects of atherosclerosis, as well as the characteristics of atherosclerotic plaque. [9-12] However, most of these studies have been carried out on subjects with different levels of coronary artery stenosis. We conducted an IVUS study on coronary arterial remodeling in patients with moderate coronary artery stenosis to determine the relationship between vascular remodeling and the plaque features of coronary atherosclerosis.
METHODS
Sample size
The study included 215 patients at Cho Ray Hospital, Ho Chi Minh City, Vietnam, who signed informed consent forms and underwent an intravascular ultrasound and coronary angiography for assessment of coronary artery disease. Data were collected for patients’ age, gender, height, weight, body mass index (BMI), body surface area (BSA), and cardiovascular risk factors.
The interpretation and the analysis of coronary angiography
Percutaneous coronary angiography was performed in the cardiac catheterization laboratory using a digital angiography system (Siemens, Germany) with an entrance to the femoral artery or with a rotary arthrotome and Seldinger's technique. Coronary angiography was performed with conventional diagnostic catheters. A contrast agent was injected into the coronary artery through a catheter, and the coronary artery was captured in different aspects to reveal the most obvious and serious lesions, the less overlapping lesions, and the unobstructed lesions. The results were stored on a CD-ROM and witnessed using an "off-line" process with the quantitative coronary analysis (QCA) software supplied with the system for consistent analysis and measurement of the coronary artery size. The stenosis diameter percentage was calculated automatically by the QCA software. Only lesions showing moderate stenosis according to diameter (which meant 40–70% stenosis for the coronary artery branches and 30–50% stenosis for the whole stem) were analyzed by IVUS.
The interpretation and the analysis of intravascular ultrasound
After coronary angiography, all patients showing lesions with moderate stenosis underwent the IVUS examination. Coronary IVUS was conducted in the cardiac catheterization laboratory using a Volcano S5 intravascular ultrasound machine (USA) with an Eagle EyeÒ Gold digital ultrasound probe with a frequency of 20 MHz. Images were saved on DVD. The built-in software system enabled automatic drawing of the edges and measurement of parameters on the IVUS image, including the lumen diameter or the size of the blood vessel and the lumen area at the coronary arteries.
Data from the IVUS examination were analyzed at three cross-sectional locations: the location with minimal lesion lumen area, the near reference position, and the remote reference position. The measured parameters included the minimum lumen area on the lesion, the total artery area, the average reference artery area (the mean of the near reference artery and the remote reference artery area), the maximum and the minimum of plaque thickness (plaque thickness plus the maximum and the minimum inner elastic lamina that was equal to the distance from the plaque surface to the inner elastic lamina), plaque area (the difference between the total artery area and the lumen area), plaque burden (Plaque area/Total artery area × 100), vascular remodeling index (the ratio between the total artery area of the lesion site and the total reference artery area), and eccentricity index (the ratio between the maximum and the minimum plaque thickness). Lesions were considered eccentric for an eccentricity index ≥ 3.0 and concentric for an index < 3.0. Remodeling was defined as positive for a remodeling index > 1.0 and negative for an index ≤ 1.0 (Figure 1).
Statistical analysis
The data were analyzed with Stata 13.0 software using medical statistical algorithms. The Kolmogorov-Smirnov test was employed to confirm a normal distribution. Continuous variables with normal distribution were presented as mean and standard deviation. Data without a normal distribution were presented as median and quartile. Categorical variables were summarized as frequencies and percentages. A t-test was used to compare two continuous variables with the normal distribution. If the distribution was not normal, the Mann Whitney test was performed. For categorical variables, comparisons were made using the Chi-squared test or Fisher’s exact test.
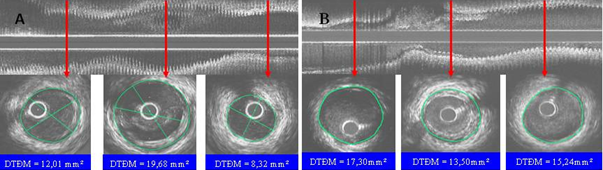
Figure 1. Positive remodeling (A) and negative remodeling (B).
RESULTS
Patient characteristics
The IVUS findings identified 88 lesions (40.9%) with positive remodeling and 127 lesions (59.1%) with negative remodeling. The characteristics of patients in these two remodeling groups are presented in Table 1. Patients in both groups were similar in age (about 60–61 years old), BMI (around 24 kg/m2), and BSA (1.68±0.17). More male patients were diagnosed with negative remodeling (88 patients) than with positive (71 patients) remodeling. However, no statistically significant differences were evident in characteristics and risk factors between the positive and negative remodeling groups (p>0.05) (Table 1).
|
Table 1. Comparisons on characteristics between positive and negative remodeling patients (N=215). |
|||
|
Variables |
Positive remodeling |
Negative remodeling |
P-value* |
|
Age (years), mean±SD |
60.85±8.83 |
60.32±10.31 |
0.691 |
|
Male, n (%) |
71 (80.7) |
88 (69.3) |
0.061 |
|
BMI (kg/m2), mean±SD |
23.86±3.24 |
24.10±3.05 |
0.571 |
|
BSA (m2), mean±SD |
1.68±0.17 |
1.68±0.17 |
0.986 |
|
Hypertension, n (%) |
58 (65.9) |
75 (59.1) |
0.309 |
|
Diabetes, n (%) |
32 (36.4) |
38 (29.9) |
0.322 |
|
Dyslipidemia, n (%) |
77 (87.5) |
106 (83.5) |
0.414 |
|
Smoking, n (%) |
30 (34.1) |
55 (43.3) |
0.174 |
* t-test and Chi-square test; BMI: Body Mass Index, BSA: Body Surface Area
Clinical characteristics
The clinical characteristics of coronary artery disease were associated with two types of coronary arterial remodeling (Table 2). The frequency of occurrence of acute coronary syndrome was significantly higher in positive remodeling than in negative remodeling (47.7% vs. 8.7%, p<0.001). The risk of acute coronary syndrome was 9.84-fold higher in patients with positive remodeling than negative remodeling (OR=9.63; 95% CI: 4.56–20.31; p <0.001).
|
Table 2. Comparisons on coronary diseases between positive and negative remodeling patients (N=215). |
|||
|
Variables |
Positive remodeling |
Negative remodeling |
P-value |
|
Acute coronary syndrome, n (%) |
42 (47.7) |
11 (8.7) |
< 0.001 OR=9.63; CI 95%: 4.56–0.31 |
|
Chronic coronary artery disease, n (%) |
46 (52.3) |
116 (91.8) |
|
Plaque characteristics
|
Table 3. Comparisons of artery symptoms between positive and negative remodeling patients (N=215). |
|||
|
Variables |
Positive remodeling (n=88) |
Negative remodeling |
P-value |
|
Minimal lumen area (mm2) |
3.97±1.50 |
4.01±1.42 |
0.830 |
|
Stenosis area (%) |
43.29±18.80 |
50.21±14.3 |
0.003 |
|
Plaque area (mm2) |
9.40±3.93 |
7.58±3.29 |
<0.001 |
|
Plaque burden (%) |
68.95±10.38 |
63.76±10.27 |
<0.001 |
|
Level of eccentricity (mm) |
3.11±1.62 |
3.25±1.59 |
0.505 |
The plaque area and plaque burden were significantly higher in patients with positive remodeling than negative remodeling (Table 3). By contrast, the stenosis area was significantly smaller for lesions with positive remodeling than negative remodeling (43.29±18.80 mm2 vs. 50.21±14.31 mm2, p=0.003). The level of eccentricity was larger in the negative than in the positive remodeling group (p=0.55). Overall, 64.8% of lesions with positive remodeling and 70.9% of the lesions with negative remodeling were eccentric. No difference was found between the two groups in terms of the level of eccentricity (p=0.345).
DISCUSSION
Arterial remodeling is a change in blood vessel size that accompanies the development of atheroma. [13, 14] At some transplant centers, one or more coronary artery branches are routinely monitored by IVUS and coronary angiograms a few weeks after a heart transplant. This is because the coronary arteries of most heart donors (who are usually young and die because of traffic accidents) frequently show atheroma by IVUS. A study by Tuzcu et al. [15] reported that more than half of the heart donors with an average age of 32 years had at least one site with an intimal thickness exceeding 0.5 mm, despite having normal coronary angiographic results. The issue of localized or diffuse lesions without stenosis on coronary angiography may cause confusion among cardiologists who still consider an injured coronary artery to be a "damaged duct". However, this designation does not seem appropriate for coronary arteries.
In 1987, Glagov et al. [4] identified an important phenomenon regarding the development of coronary atherosclerotic lesions at an early stage. They recruited 136 hearts obtained at autopsy to examine whether the enlargement of atherosclerotic human coronary arteries was correlated with the lesion area. They found a positive correlation between the area of the internal elastic lamina area and the area of the lesion (r=0.44, p<0.0001). If the percentage of stenosis was less than 40%, the size of the blood vessels caused an excessive deposition of atheroma, which led to an increased lumen area. The level of coronary arterial remodeling was less obvious than with severe lesions (above 40% stenosis), so the lumen area was markedly diminished. Therefore, the authors concluded that coronary arterial remodeling was the mechanism for the compensatory enlargement that maintained the lumen size. In addition to the 40% stenosis, the diameter of the lumen decreased following the progression of diseases related to coronary artery progression. Glagov's discovery was later evaluated by IVUS.
In recent years, various studies on ultrasound have demonstrated a new aspect of the remodeling called negative remodeling. [5, 11, 12] At the lesion site, the area of the external elastic lamina can decrease considerably, which results in stenosis instead of a compensatory enlargement. This negative remodeling was initially described in arterial stenosis after coronary intervention. Moreover, it was also found in lesions with moderate stenosis of the coronary arteries. A relationship between positive and negative remodeling has not been identified. One hypothesis is that positive remodeling occurs in the early stage of atherosclerosis, whereas negative remodeling appears in the final stage. [16, 17] Therefore, negative remodeling is more frequently observed in severe lesions than in non-critical lesions. In our study, the proportion of the stenosis area was lower in the positive remodeling group than in the negative remodeling group, even though both groups had similar lumen areas.
The mechanism of arterial remodeling still has not been clarified. [14] Systemic and local factors may affect arterial remodeling. Tauth et al., [18] in a study of 67 patients, emphasized that smoking was associated with negative remodeling, while hypercholesterolemia was associated with positive remodeling. Likewise, Weissman et al. [19] also highlighted that smoking was the only risk factor associated with negative remodeling. Hamasaki et al. [20] conducted a clinical trial of 101 patients with normal or mildly diseased coronary arteries and showed that cholesterol-lowering treatment influenced positive remodeling by an increase in vessel area, as determined by coronary angiography. Our findings indicated a higher prevalence of smoking in the negative remodeling than in the positive remodeling group. By contrast, dyslipidemia was greater in patients with positive remodeling than negative remodeling. However, these differences were not statistically significant.
Ishida et al. [21] demonstrated a significant positive correlation between age and plaque area and vessel area in a study of 26 patients with normal and mildly diseased coronary arteries and without coronary risk factors. By contrast, Hirose et al. [22] found no correlation between risk factors and types of coronary arterial remodeling. In our study, the risk factors showed no statistically significant differences between the two groups of coronary arterial remodeling, except that the percentage of men was significantly higher in the positive remodeling than in the negative remodeling group.
Although the mechanism of positive and negative remodelings has not been defined precisely, these phenomena have important impacts on clinical evaluation. The observation of positive remodeling observed on coronary angiography was an essential factor in the assessment of the severity of atherosclerosis. Therefore, blood vessels would contain a large atheroma but slight stenosis if the vascular remodeling was able to compensate for the atheroma. Our results were consistent with this idea. Recent evidence has suggested that remodeling sites tend to be prone to plaque rupture. In other words, positive remodeling was more common in unstable patients, while negative restructuring was more common in stable patients. Schoenhagen et al. [23] used IVUS to evaluate 86 patients with unstable and 46 patients with stable coronary syndrome and reported that positive remodeling and a larger plaque area were associated with unstable angina. During pregnancy, negative remodeling was more frequent in stable angina.
The combination of the types of remodeling and clinical characteristics may reflect a greater predisposition for an atheroma with a positive remodeling to cause acute coronary syndrome. Jeremias et al. [12] illustrated that positive remodeling was observed in 65% in patients with unstable coronary syndromes, while the corresponding figure was only 9% in those with stable angina (p<0.001).
CONCLUSION
The types of coronary arterial remodeling were associated with different clinical characteristics. Positive remodeling was more common in acute coronary syndrome than in stable angina. The plaque area was larger and the plaque burden was higher for positive remodeling than for negative remodeling of lesions with moderate stenosis. Nevertheless, the compensatory enlargement in the positive remodeling group still ensured a lower level of stenosis, despite the same lumen area between the two groups.
ACKNOWLEDGMENT
The authors acknowledge the support from Cho Ray Hospital for implementation of the study. They also express their deepest gratitude to all the patients for their contribution to this research.
Conflict of interest
The authors declare that they have no conflict of interest.
REFERENCES
- Zaazaa AM. Celery (Apium graveolens) ethanolic extract ameliorates experimental atherosclerosis in rats. International Journal of Pharmaceutical and Phytopharmacological Research. 2018; 8(4):28-4
- National Heart Lung and Blood Institute, Atherosclerosis, [Online]. Available: https://www.nhlbi.nih.gov/health-topics/atherosclerosis. [Accessed: 23rd Dec, 2019].
- Linawati NM, Sriwidyani NP, Wande IN, Kamasan A, Wiryawan S, Ratnayanti D, Sugiritama W, Wahyuniari I. The combination extract of pare and apples (APa) reduces risk of atherosclerosis through reduction of interleukin 17 and aggregate focus of liver inflammation in high-fat diet mice. International Journal of Pharmaceutical and Phytopharmacological Research. 2018; 8(4):63-69.
- Glagov S, Weisenberg E, Zarins CK, Stankunavicius R, Kolettis GJ. Compensatory enlargement of human atherosclerotic coronary arteries. N. Engl. J. Med. 1987; 316:1371–1375.
- Smits PC, Bos L, Quarles van Ufford MA, Eefting FD, Pasterkamp G, Borst C. Shrinkage of human coronary arteries is an important determinant of de novo atherosclerotic luminal stenosis: an in vivo intravascular ultrasound study. Heart. 1998; 79:143–147.
- von Birgelen C, Mintz GS, de Vrey EA, Kimura T, Popma JJ, Airiian SG, Leon MB, Nobuyoshi M, Serruys PW, de Feyter PJ. Atherosclerotic coronary lesions with inadequate compensatory enlargement have smaller plaque and vessel volumes: observations with three dimensional intravascular ultrasound in vivo. Heart. 1998; 79:137–142.
- Garcia-Garcia H, Costa M, Serruys P. Imaging of coronary atherosclerosis: Intravascular ultrasound. Eur. Heart J. 2010; 31:2456–2469.
- Hartmann M, Huisman J, Böse D, Jensen LO, Schoenhagen P, Mintz GS, Erbel R, von Birgelen C. Serial intravascular ultrasound assessment of changes in coronary atherosclerotic plaque dimensions and composition: an update. Eur. J. Echocardiogr. 2011; 12:313–321.
- Ward MR, Jeremias A, Hibi K, Herity N, Lo S, Filardo S, Lee DP, Fitzgerald PJ, Yeung AC. The influence of plaque orientation (pericardial or myocardial) on coronary arterial remodeling. Atherosclerosis. 2001; 154:179–183.
- Varnava AM, Mills PG, Davies MJ. Relationship between coronary artery remodeling and plaque vulnerability. Circulation. 2002; 105:939–943.
- Gyongyosi M, Yang P, Hassan A, Weidinger F, Domanovits H, Laggner A, Glogar D. Arterial remodelling of native human coronary arteries in patients with unstable angina pectoris: a prospective intravascular ultrasound study. Heart. 1999; 82:68–74.
- Jeremias A, Spies C, Herity NA, Pomerantsev E, Yock PG, Fitzgerald PJ, Yeung AC. Coronary artery compliance and adaptive vessel remodelling in patients with stable and unstable coronary artery disease. Heart. 2000; 84:314–319.
- Burke AP, Kolodgie FD, Farb A, Weber D, Virmani R. Morphological predictors of arterial remodeling in coronary atherosclerosis. Circulation. 2002; 105:297–303.
- Gibbons GH, Dzau VJ. The emerging concept of vascular remodeling. N. Engl. J. Med. 1994; 330:1431–1438.
- Tuzcu EM, Kapadia SR, Tutar E, Ziada KM, Hobbs RE, McCarthy PM, Young JB, Nissen SE. High prevalence of coronary atherosclerosis in asymptomatic teenagers and young adults: evidence from intravascular ultrasound. Circulation. 2001; 103:2705–2710.
- Schoenhagen P, Ziada KM, Vince DG, Nissen S, Tuscu EM. Arterial remodeling and coronary artery disease: the concept of "dilated" versus "obstructive" coronary atherosclerosis. J. Am. Coll. Cardiol. 2001; 38:297–306.
- Ward MR, Pasterkamp G, Yeung AC, Borst C. Arterial remodeling. Mechanisms and clinical implications. Circulation. 2000; 102:1186–1191.
- Tauth J, Pinnow E, Sullebarger JT, Basta L, Gursoy S, Lindsay J Jr, Matar F. Predictors of coronary arterial remodeling patterns in patients with myocardial ischemia. Am. J. Cardiol. 1997; 80:1352–1355.
- Weissman NJ, Sheris SJ, Chari R, Mendelsohn FO, Anderson WD, Breall JA, Tanguay JF, Diver DJ. Intravascular ultrasonic analysis of plaque characteristics associated with coronary artery remodeling. Am. J. Cardiol. 1999; 84:37–40.
- Hamasaki S, Higano ST, Suwaidi JA, Nishimura RA, Miyauchi K, Holmes DR Jr, Lerman A. Cholesterol-lowering treatment is associated with improvement in coronary vascular remodeling and endothelial function in patients with normal or mildly diseased coronary arteries. Arterioscler. Thromb. Vasc. Biol. 2000; 20:737–743.
- Ishida S, Hamasaki S, Kamekou M, Yoshitama T, Nakano F, Yoshikawa A, Kataoka T, Saihara K, Minagoe S, Tei C. Advancing age is associated with diminished vascular remodeling and impaired vasodilation in resistance coronary arteries. Coron. Artery. Dis. 2003; 14:443–449.
- Hirose M, Kobayashi Y, Mintz GS, Moussa I, Mehran R, Lansky AJ, Dangas G, Kreps EM, Collins MB, Stone GW, Colombo A, Leon MB, Moses JW. Correlation of coronary arterial remodeling determined by intravascular ultrasound with angiographic diameter reduction of 20% to 60%. Am. J. Cardiol. 2003; 92:141–145.
- Schoenhagen P, Ziada KM, Kapadia SR, Crowe TD, Nissen SE, Tuzcu EM. Extent and direction of arterial remodeling in stable versus unstable coronary syndromes: an intravascular ultrasound study. Circulation. 2000; 101:598–603.
