Archive \ Volume.14 2023 Issue 4
Adherence and Health-related Quality of Life of Transfusion-Dependent Thalassemia Patients
Lee Wan Jin1, Nurul Ain Mohd Tahir1*, Farida Islahudin1, Li Shu Chuen2
1Faculty of Pharmacy, Universiti Kebangsaan Malaysia, Jalan Raja Muda Abdul Aziz, 50300 Kuala Lumpur, Malaysia. 2School of Biomedical Sciences and Pharmacy, University of Newcastle, Callaghan, New South Wales, Australia.
Abstract
Adherence to iron chelation therapy (ICT) is fundamental for preventing iron overload complications and maintaining health-related quality of life (HRQoL) in transfusion-dependent thalassemia (TDT) patients. This study aimed to evaluate adherence, HRQoL, and their association among Malaysian TDT patients. Cross-sectional research was performed among TDT patients aged 18 years and above in Hospital Ampang, Selangor. The adherence and the HRQoL (SF-36) were evaluated using validated instruments. Correlation analyses were carried out to determine the association between ICT adherence and HRQoL. The study recruited 162 patients, with 46.91% (N=76) of respondents reporting being adherent. The mean SF-36 score for TDT patients is 74.58. Remarkably, adherent patients exhibit significantly higher HRQoL (mean SF-36 score 79.21) assessed by the SF-36 questionnaire versus nonadherent patients (mean SF-36 score 69.47) (p=0.00). The findings also revealed a significant positive correlation between female (p=0.032), employed (p=0.003), and age (p=0.050) factors with the patient’s HRQoL. The rate of ICT adherence for adult TDT patients is suboptimal and non-adherent to ICT has significantly compromised HRQoL. Enhancing the rate of ICT adherence through interventions such as patient counseling and support programs may lead to enhanced HRQoL outcomes for the TDT population.
Keywords: Transfusion-dependent thalassemia (TDT), Iron chelation therapy (ICT), Health-related quality of life (HRQoL), Short form 36 (SF-36), Adherence
INTRODUCTION
Iron chelation therapy (ICT) adherence is a major determinant of optimal iron overload management in transfusion-dependent thalassemia (TDT) patients, and it deserves much better clinical attention [1]. In clinical practice, medication adherence refers to the extent of compliance with the healthcare provider’s treatment recommendation concerning frequency, dosage, and schedule [2]. Many factors could lead to nonadherence to medications [3], hence, healthcare providers should assess the patient’s medication adherence periodically in order to assist in addressing patients’ concerns regarding the medications [4]. This will prevent the physicians from underestimating the therapeutic effects and subsequently lead to unnecessary treatment regimen modification [5]. In addition, in TDT patients, high ICT adherence has many associated health benefits such as lesser iron accumulation and a lower risk of iron overload complications such as cardiac, liver, and endocrinologic morbidities [6-10].
The progression of thalassemia disease, the risk of iron-related complications, the frequent hospitalization, and the high medical costs have a deleterious impact on patients' lives and result in significantly reduced health-related quality of life (HRQoL). Therefore, HRQoL should be monitored routinely as an important and complementary index of effective treatment in thalassemia patients. According to the Centers for Disease Control and Prevention (CDC), the term “HRQoL” generally refers to a multidimensional evaluation of the impact of disease and treatment on a patient’s perception of overall function and well-being. It was reported thalassemia patients have struggled with psychological and social behavior problems such as low self-esteem, tension, depressive symptoms, anxiety, weak social skills, and poor academic performance [11]. This was further confirmed by a meta-analysis of 26 studies involving up to 687 patients worldwide showing beta-thalassemia disease had a significant negative impact on the patient’s HRQoL, especially in general physical health and social functioning [12]. This decline in HRQoL was further aggravated among nonadherent patients affecting their social, mental, and physical conditions [13].
Numerous studies have been conducted worldwide to assess HRQoL using SF-36 in beta-thalassemia patients, however, limited information on the association between chelation adherence and HRQoL was available [12]. More comprehensive research to gain a better understanding of the impact of chelation adherence on patients’ HRQoL would enable healthcare providers to optimize care and tailor interventions to the needs of thalassemia patients. Thus, the overall aim of this study was to evaluate ICT adherence, HRQoL, and their association with TDT patients in Malaysia. By comparing HRQoL among adherent and nonadherent groups, this study would provide clinical evidence of the significance of adherence in thalassemia management, and suggestions to develop integrated strategies for the best possible patient care.
MATERIALS AND METHODS
Study Design
This was a cross-sectional, questionnaire-based study performed at Hospital Ampang, Selangor which serves as the main hematology center in Malaysia. Convenient sampling was used for data collection from 1st August 2021 to 30th December 2021, with informed consent obtained from all eligible individuals prior to engaging in any study-related activity. In order to reduce selection bias, the researchers were blinded to the patient's clinical features, such as type of ICT, serum ferritin level, and iron overload status, at the time of questionnaire administration.
Inclusion and Exclusion Criteria
Patients aged 18 years and older with a diagnosis of transfusion-dependent thalassemia (TDT), treated with at least one iron chelation therapy (ICT), and able to speak, read, and understand Malay and English were recruited for the study. Patients with comorbidities of sickle cell disease (SCD), myelodysplastic syndrome (MDS), and other hematologic diseases were excluded. Besides, the patient who had just begun their follow-up in Hospital Ampang or had incomplete clinical data during the study period were excluded.
Sample Size Estimation
The sample size in this study was calculated by using a single proportion formula through Raosoft © calculator [14]. With an absolute precision set at 0.05, a confidence level of 95%, and a Malaysian TDT population of 4529. The proportion of nonadherence to iron chelation therapy of 0.086 was used based on the study by Lam et al. (2021) [15]. The calculated sample size was 118, and accounting for 10% of non-respondents, a minimal sample size of 135 was required.
Data Collection
Eligible TDT patients were approached and invited to participate in this study. A detailed explanation of the study’s objectives and procedures was given to the patients, and written consent was obtained prior to the study. The questionnaires were available in English and Malay and consisted of three sections: Section 1 involved demographic information including race, gender, body weight, marital status, employment status, age of thalassemia diagnosis, and types of ICT. The researchers also collected the relevant clinical data of the baseline serum ferritin levels during the data collection period retrospectively using the electronic Health Informatics System (eHIS), the institution’s electronic medical records.
Section 2 of the questionnaires involved measuring the adherence rate among the participants using the Malaysia Medication Adherence Assessment Tool (MyMAAT) [4]. It is made up of 21 questions under preliminary constructs of patients’ attitudes towards taking medication, their perception of the medicine’s utility in terms of benefits, cost, efficacy, barriers, severity, and susceptibility to disease, patients’ sociocognitive theory, and others. Each question was scored from one to five. The patient’s adherence status was then classified using the cut-off point of 54, for instance, scores 12-53 indicated non-adherence while scores 54-60 indicated adherence. Meanwhile, section 3 included a questionnaire to measure patients’ health-related quality of life (HRQoL) using the SF 36 health survey tool [16, 17]. The tool evaluated the domains of physical function (PF), role limitations caused by physical unwellness (RP), role limitations due to emotional problems (RE), vitality (VT), mental health (MH), social function (SF), bodily pain (BP) and general health (GH). Each domain has a score between 0 and 100, with higher scores denoting better well-being and health.
Statistical Analysis
All data analyses were conducted using SPSS (Statistical Package for the Social Sciences) version 21.0. Descriptive statistics were applied to analyze patients’ demographic data, clinical data, adherence, and mean SF-36 scores. Continuous data were presented in mean and standard deviation, while categorical data were presented in frequency and percentage. The Kolmogorov-Smirnov test was then performed to determine the normality of the data. The outcome variables were two-fold; patient’s adherence status (nominal variable) and mean SF-36 score which served as a measure of patient’s health-related quality of life (HRQoL) (scale variable). As the data was found skewed, the correlation between patient adherence and serum ferritin levels was identified by using the Mann-Whitney test with a significance value of p < 0.05. The correlation of adherence and types of ICT, monotherapy, or combination of ICT were determined using a chi-square test. Only the potential factors with p values <0.05 were reported to have a significant association with patient adherence. Besides that, Mann-Whitney and Kruskal-Wallis tests are used to determine to association between patients’ HRQoL and potential factors such as adherence, gender, ethnicity, marital status, working status, age, monotherapy, or combination of ICT, and injectable or non-injectable ICT using a significant p value <0.05. To further investigate the differences between age categories and HRQoL, a post hoc analysis of the Kruskal-Wallis test was performed to determine the pairwise comparisons
RESULTS AND DISCUSSION
Overall, 209 sets of questionnaires were distributed and completed. However, only 162 patients fulfilled the criteria, with 31 patients excluded due to incomplete clinical data, 10 repeated patients, 4 non-transfusion dependent thalassemia patients, one patient did not follow up in the specified hospital, and the data of one patient not traceable in eHIS.
Demographic and Clinical Characteristics
The demographic and clinical characteristics of enrolled participants and their classification into adherent and nonadherent groups were summarized. (Table 1). Most of the participants were Malay (N=115, 70.99%) followed by Chinese (N=43, 26.54%). Approximately, two-thirds of the subjects were female (N=107, 66.05%). The subjects in this study ranged in age from 18 to 72 years, with a mean age of 32.88 years (SD = 10.45). More than half of them (N=87, 53.7%) were single, and most (N=112, 69.14%) were employed. The adherent patients had significantly lower serum ferritin levels (with U = 1774, p<0.001).
|
Table 1. Demographic and clinical characteristics of transfusion-dependent thalassemia patients according to their adherent status |
|||
|
Total number of participants (N=162), (N,%) |
Adherent patients (N=76) (N,%) |
Non adherent patients (N=86) (N,%) |
|
|
Age (year), mean (SD) |
32.88 (10.45) |
35.12 (11.80) |
30.91 (8.69) |
|
Age category |
|
|
|
|
Young adult (18- 25 years) |
46 (28.40%) |
18 (23.68%) |
28 (32.56%) |
|
Adult (26- 44 years) |
91 (56.17%) |
41 (53.95%) |
50 (58.14%) |
|
Middle age (45- 59 years) |
22 (13.58%) |
14 (18.42%) |
8 (9.30%) |
|
Old age (≥60 years) |
3 (1.85%) |
3 (3.95%) |
- |
|
Race |
|||
|
Malay |
115 (70.99%) |
49 (64.47%) |
66 (76.74%) |
|
Chinese |
43 (26.54%) |
26 (34.21%) |
17 (19.77%) |
|
Indian |
1 (0.62%) |
0 (0%) |
1 (1.16%) |
|
Others |
3 (1.85%) |
1(1.32%) |
2 (2.33%) |
|
Gender |
|||
|
Female |
107 (66.05%) |
50 (65.79%) |
57 (66.28%) |
|
Male |
55 (33.95%) |
26 (34.21%) |
29 (33.72%) |
|
Marital Status |
|
|
|
|
Married |
73 (45.06%) |
36 (47.37%) |
37 (43.02%) |
|
Single |
87 (53.70%) |
39 (51.32%) |
48 (55.81%) |
|
Divorced |
2 (1.24%) |
1 (1.31%) |
1 (1.17%) |
|
Employed |
112 (69.14%) |
57 (75%) |
55 (63.95%) |
|
Not employed |
50 (30.86%) |
19 (25%) |
39 (45.35%) |
|
Type of Thalassemia |
|||
|
Beta-thalassemia major |
57 (35.19%) |
30 (39.47%) |
27 (31.40%) |
|
Haemoglobin E beta thalassemia |
79 (48.77%) |
31 (40.79%) |
48 (55.81%) |
|
Haemoglobin H disease |
15 (9.25%) |
10 (13.16%) |
5 (5.81%) |
|
Beta-thalassemia intermediate |
10 (6.17%) |
5 (6.58%) |
5 (5.81%) |
|
Others |
1 (0.62%) |
0 (0%) |
1 (1.17%) |
|
Mean Body weight (kg), SD |
51.81 (7.59) |
53.22 (7.63) |
50.56 (7.38) |
|
Average serum ferritin (ng/mL), SD |
3111.22 (2857.53) |
2103.15 (1973.63) |
4002.07 (3212.15) |
Adherence to Iron Chelation Therapy (ICT)
In total, the adherence rate to iron chelation therapy (ICT) was 46.91%. An independent chi-square test found a significant relationship between ICT type and adherence, Χ2(4) =7.69, p =.048. Patients on monotherapy (N=78) adhered at a rate of 52.56%, while patients on combination therapy (N=82) adhered at a rate of 41.67% (Table 2) demonstrated non-significant association with Χ2(1) =1.93, p =.165. Adherence rates for patients prescribed with injectable ICT (36.36%) were lower than for those provided with the combination of injectable and oral ICT (41.67%) and oral ICTs (55.22%) with Χ2(2) =3.59, p =.166.
|
Table 2. The number and proportion (%) of patients adherent to iron chelation therapy (ICT) by treatment type |
|||
|
Total participants, (N) |
Adherent Patients, N (%) |
Nonadherent patients, N (%) |
|
|
Total (N) |
162 |
76 (46.91%) |
86 (53.10%) |
|
Monotherapy |
78 |
41 (52.56%) |
37 (47.44%) |
|
DFO |
11 |
4 (36.36%) |
7 (63.64%) |
|
DFP |
62 |
32 (51.61%) |
30 (48.39%) |
|
DFX |
5 |
5 (100%) |
0 |
|
Combination |
84 |
35 (41.67%) |
49 (58.33%) |
|
DFO&DFP |
82 |
34 (41.46%) |
48 (58.54%) |
|
DFO&DFX |
2 |
1 (50%) |
1 (50%) |
|
Injectable ICT |
11 |
4 (36.36%) |
7 (63.64%) |
|
Combination of injectable and oral ICT |
84 |
35 (41.67%) |
49 (58.33%) |
|
Non-injectable ICT |
67 |
37 (55.22%) |
30 (44.78%) |
ICT: iron chelation therapy; DFO: desferrioxamine; DFP: deferiprone; DFX: deferasirox
Health-related Quality of Life (HRQoL)
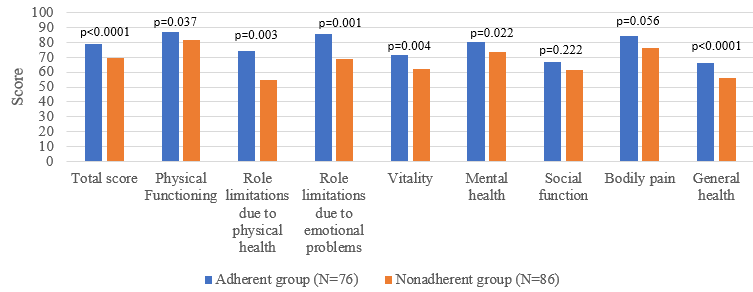
The overall SF36 score and the scores of the eight domains were summarized and compared among adherent and nonadherent groups (Figure 1). TDT patients had an average total SF-36 score of 74.58, with physical functioning (PF) scoring the highest at 84.57 and general health (GH) scoring the lowest at 60.71. The adherent patient had a significantly higher score in overall and every aspect of HRQoL compared to the nonadherent patient, except in the domains of social function (SF) and bodily pain (BP) (Figure 1). The average SF36 score for the adherent group was 79.21, with domains ranging from 66.47 for general health (GH) to 87.04 for physical functioning (PF) respectively. The nonadherent group's average SF36 score was 69.47, with the role limitations due to physical health (RP) and physical functioning (PF) domains scoring the lowest at 54.94 and highest at 81.40 respectively.
|
|
|
Figure 1. The 36-Item Short Form Survey scores and its domains between adherent and nonadherent groups of transfusion-dependent thalassemia (TDT) patients with p-value (Mann-Whitney U test) |
For factors associated with HRQoL, the findings indicated that gender, working status, patients’ adherence to ICT, and age were significant factors affecting the patient’s HRQoL, with p=0.032, p=0.003, and p=0.000 respectively. Females, unemployed, and patients with lower ICT adherence all had a significantly lower HRQoL. The Kruskal-Wallis test revealed significant variation among age categories (with Χ2(3) = 7.82, p <0.05), while the post hoc analysis of Kruskal-Wallis test assessing the pairwise comparisons of age category on HRQoL demonstrated young adults (aged 18-25) and adults (aged 26-44) exhibited significantly higher HRQoL scores than those in the older age group (aged ≥60) with p=0.026 and p=0.016 respectively
In this study, the association between ICT adherence and patients with transfusion-dependent thalassemia (TDT) HRQoL was comprehensively examined. To acquire an in-depth understanding, this study investigated two key areas: first, it evaluated the rate of ICT adherence specifically among adult TDT patients in Malaysia. Second, it examined the effect of patients’ ICT adherence on their HRQoL. This approach ensured a holistic examination of the impact of adherence on the health outcomes of TDT patients. The study revealed a substantial rate of nonadherence towards ICT of 53.09% among adult TDT patients in Malaysia, highlighting a key issue that requires special attention.
Meanwhile, the established application of the Short Form-36 Health Survey (SF-36) in beta-thalassemia patients [12] would support its suitability for evaluating HRQoL among the TDT population and allow international comparison. To the best of our knowledge, a limited number of studies were performed worldwide to assess the impact of adherence on HRQoL in TDT patients. The results of this cross-sectional study also revealed evidence of the relationship between ICT adherence and HRQoL. Notably, patients with lower adherence had impaired and lower HRQoL.
The adherence rate to ICT reported using MyMAAT in this study was comparable to the rates reported worldwide which ranged from 20.93% to 75.3% [7, 8, 18, 19]. The controversy and debate on the definition of adherence and the appropriate ways to quantify it are the main factors contributing to the variability in the reported adherence rates [20]. Oral chelators such as DFP and DFX tend to have a higher adherence rate than injectables DFO, comparable to multiple previous studies. The rates of adherence to oral chelators were higher, ranging between 87.2-100% [8, 21, 22]. As compared to injectables chelators ranged from 48.84 to 85.1% [10, 23-29]. This discrepancy in compliance demonstrates that issues such as inconvenience, uncomfortable administration, and side effects especially associated with parenteral administrations contribute to the adherence rate [30]. This study’s results demonstrated that the types of ICT had a statistically significant impact on patient adherence rates. However, interestingly, despite the oral ICT having a higher adherence rate, it was not found to be significantly superior to injectable ICT and a combination of injectable and oral ICT in terms of adherence in our study.
The findings of this study with respect to the significant positive association of adherence and HRQoL were similar to a previous study in Malaysia that TDT patients on an optimal DFO dosage (which indirectly reflected higher adherence), had higher QoL scores than those on a sub-optimal DFO dosage [31]. Furthermore, the study conducted by Haghpanah et al. (2013) also reported that patients who adhered to ICT exhibited significantly improved HRQoL compared to those with poor ICT adherence. Notably, the adherent patients had a significantly higher than those categorized as poor adherent patients. The similarity of these studies collectively emphasizes the importance of ICT adherence in enhancing the HRQoL of TDT patients. Positive attitudes and perceptions of patients who had better medication adherence may lead to better handling of disease-related issues [25]. This could be the reason why they had higher HRQoL especially enhanced physical function, reduced role limitation due to physical function, increased vitality, and better general health in this study. Furthermore, the improved TDT management of adherent patients results in them feeling at ease and less anxious, eventually leading to an improvement in their mental health and fewer difficulties with their everyday obligations brought on by emotional distress. However, our study showed no significant difference in bodily pain and social function of HRQoL between adherent and nonadherent patients. This result might be attributed to the fact that patients with thalassemia often experience fatigue, chronic pain, and discomfort due to the inherent anemia and regular blood transfusions. The iron accumulation due to repeated blood transfusions may cause asthenia and body weakness in some patients, frequently accompanied by both joint and abdominal pain [32]. he bodily pain and fatigue they are suffering could potentially drain their energy and reduce their ability to engage socially.
While age is often considered a significant predictor of HRQoL [25, 33], our study also indicated significant disparities in HRQoL across different age groups. Generally, young adults and adults typically have greater physical health and vitality compared to older adults. As individuals age, they become more susceptible to various health issues and chronic diseases, which might negatively affect their HRQoL. Additionally, older adults may experience social isolation as a result of retirement, the loss of friends and family, and restricted mobility, resulting in a potential decline in their physical performance and HRQoL [34]. These would partially account for the lower HRQoL in addition to the impact of nonadherence. Female gender is commonly recognized as a contributing factor to lower HRQoL scores [33, 35]. In our study, the HRQoL of TDT women was significantly lower compared with the HRQoL of men with TDT, including aspects of physical health, role limitations because of physical function, social activity, and body pain. Women may overstate their worse health status during health self-reports, but studies have shown that women struggle with psychological disorders at a higher rate than men in the general population [36]. Furthermore, Women also tend to suffer from compromised HRQoL as they have multiple obligations because they are generally in charge of taking care of their children and household [37]. The current study also demonstrated that employed thalassemia patients had a significantly higher HRQoL. This finding is congruent with other studies showing employment status had a positive impact on HRQoL in patients with various diseases [38, 39]. Financial security can greatly decrease the anxiety and stress related to financial expenses and directly impacting overall well-being [40]. Overall, these three factors would have contributed to the impact of adherence to HRQoL in various extent.
There are some limitations identified in the study. First, it was small-scale research conducted in a single center in Malaysia. A single-center study generally lacks the scientific rigor or external validity needed to support widespread modifications in practice. However, this is partially overcome by the status of Ampang Hospital as a major hematology center in Malaysia as it has access to a large TDT patient cohort and specialization in TDT. Secondly, the adherence and HRQoL data were assessed through patients’ self-reporting. Patients may exaggerate or under-report their severity and symptoms unconsciously. Besides, patients could experience recall bias during data collection. However, these are intrinsic and difficult to address problems with this type of study. Also, it was difficult to retrieve additional clinical parameters, such as the MRI T2* for the heart and liver, that could have been used to better determine the severity of the iron overload due to costly procedures. During the data collection process, not all patients had access to or had more than one reading of MRI T2* for the heart and liver, making it impossible to compare cardiac and liver iron load.
Given the inadequate adherence rate to ICT among TDT patients in Malaysia, several suggestions for improving adherence could be implemented in the future. The conventional education regarding thalassemia was focused on knowledge sharing about the disease, medication, and techniques for administering DFO. Healthcare professionals however tend to neglect the mental health and emotional state of TDT patients due to the medical, financial, and psychosocial burden. Countless numbers for blood transfusion, follow-up with doctors, administering DFO, or taking oral iron chelators make patients’ attitudes about adherence fluctuate over time. This highlights the importance of incorporating pragmatic self-management interventions as proposed by the World Health Organization, to enable people with chronic illnesses to manage their mental and physical health [41]. Apart from that, a previous study [1] revealed the significance of role models in patient groups. In this regard, the implementation of a specialized multidisciplinary adherence program that incorporates health coaching activities may be advantageous.
Furthermore, building a good rapport between a thalassemia patient and a healthcare professional is fundamental to encouraging the patient’s adherence to ICT for optimal therapy outcomes [1, 42]. The patient-healthcare professional connection is generally defined as a fiduciary relationship. Having a good patient-healthcare practitioner relationship allows patients to address their concerns about the disease and medicine, keeping them motivated and overcoming the challenges of adherence and persistence with ICT eventually improving their well-being. Healthcare professionals such as physicians, pharmacists, and nurses should always review their practices to avoid condescending behavior that would impede rapport-building and incorporate concerted efforts to strengthen their bond.
CONCLUSION
In conclusion, our study demonstrated suboptimal adherence to ICT among TDT patients in Malaysia. Furthermore, nonadherence to ICT was shown to significantly decrease the overall HRQoL in TDT patients except in bodily pain and social function. Besides, factors such as gender, working status, and age were found to affect the patient’s HRQoL significantly. Therefore, it is imperative to prioritize ICT adherence, as better adherence directly improves the quality of life and health outcomes for individuals with TDT. Healthcare professionals should implement personalized care plans that consider the unique demands and influencing factors of each patient to improve adherence.
ACKNOWLEDGMENTS: None
CONFLICT OF INTEREST: None
FINANCIAL SUPPORT: The funding for this paper is provided by the University Kebangsaan Malaysia by the Geran Universiti Penyelidikan (GUP-2020-003), and part of this research is supported by the Fundamental Research Grants Scheme [FRGS/1/2020/SS02/UKM/02/5] funded by the Ministry of Higher Education (MOHE), Malaysia.
ETHICS STATEMENT: The study has obtained approval from both the Medical Research Ethics Committee of the Ministry of Health Malaysia (NMRR-20-2814-57565) and the Research Ethics Committee of the National University of Malaysia (UKM PPI/111/8/JEP-2022-231).
