Archive \ Volume.11 2020 Issue 1
Trends in the Use of Surgical Antibiotic Prophylaxis
at a Provincial Hospital in Vietnam
Cang Trung Huynh 1, Tram Thi Huyen Nguyen 2, Trung Quang Vo 3*, Thao Thi Quy Le 3, Thoai Dang Nguyen 3, Son Hong Nguyen 4, Tro Van Chau 3, Sy Van Hoang 5
1 Tay Do University, Can Tho City 900000, Vietnam. 2 Ear-Nose-Throat Hospital in Ho Chi Minh City, Ho Chi Minh City 700000, Vietnam.
3 Pham Ngoc Thach University of Medicine, Ho Chi Minh City 700000, Vietnam. 4 175 Hospital, Ho Chi Minh City 700000, Vietnam.
5 University of Medicine and Pharmacy at Ho Chi Minh City, Ho Chi Minh City 700000, Vietnam.

Abstract
Background: Surgical site infection (SSI) is one of the most significant causes of patient morbidity and mortality. Although antibiotic prophylaxis is crucial to the prevention of infection in different types of surgery, there is little evidence supporting the effectiveness of using prophylactic antibiotics at the hospital. Objective: The purpose of this study was to assess trends in the use of antibiotic prophylaxis for SSI prevention at the hospital. Methods: A retrospective study was performed at Nguyen Dinh Chieu Hospital using an analysis of all surgical records from January to September 2019. The analysis comprised 407 records that met all of the criteria. Data were collected according to socio-demographic characteristics, the clinical presentation of patients with surgical treatment, and trends in using surgical antibiotic prophylaxis. Results: Patients enrolled in the study had an average age of 35.2±14.4 years and over half were female (60.7%). Only 0.7% of patients were diagnosed with superficial incisional SSI and no patients were found to be infected with other types of SSI such as deep incisional SSI, organ/space SSI or remote infection. Of 2722 treatments with prophylactic antibiotics, the most common antibiotics used were Amoxicillin/Sulbactam (28.5%) and Metronidazole (27.6%). The majority of patients were given single antibiotic therapy (58.4%) and drugs were administrated via intravenous injection (60.7%). Most prophylactic antibiotics were prescribed at the usual dose and the first dose was usually administered within an hour after surgery (66.1%). Conclusion: The use of surgical antibiotic prophylaxis at the hospital was not based on the recommendations of clinical practice guidelines. Guidelines for the prevention of SSI should be strictly followed at the hospital.
Keywords: Antibiotic, infections, hospital, province, Vietnam.

INTRODUCTION
Surgical site infections (SSIs) are thought to result in common and serious complications at the hospital and have become the most frequent cause of death among patients following surgery, worldwide [1, 2]. According to the Centers for Disease Control and Prevention (CDC) and the Healthcare Infection Control Practices Advisory Committee (HICPAC), SSIs can be incisional, organ or operative space infections that occur after surgery [3]. SSIs are also defined as those that occur at the site of the skin or deep tissue of the incision within 30 days of a surgical procedure or within 90 days if prosthetic materials are implanted at the operation [4]. The occurrence of SSI varies widely depending on the type and frequency of the surgical procedure, wound cleanliness, and operative context. Patients with SSI have a 2- to 11-fold increased risk of mortality compared to those without SSI [5]. SSI complications potentially trigger increasing morbidity rates, prolonged hospitalization, and an additional financial burden on both patients and the healthcare system [1].
A systematic literature review conducted by the World Health Organization (WHO) shows that the pooled prevalence of overall SSIs was approximately 11.2 per 100 surgical patients (95% CI: 9.7–12.8) across incidence/prospective studies over the period from 1995 to 2015 [1]. In a large-scale study that recruited 850,000 general surgeries from all across the United States, the incidence of SSIs was only 1.9% [6]. Another systematic literature review and meta-analysis of the burden of healthcare-associated infection (HAI) revealed that the pooled incidence of SSI in Southeast Asia was estimated at around 7.8% (95% CI: 6.3–9.3%). The associated mortality and increased length of hospital stay among infected patients ranged from 7% to 46% and 5 to 21 days, respectively [7]. Also, SSI is the most costly type of HAI with an estimated cost of $3.3 billion per year and is associated with nearly one million additional days for inpatients annually [8, 9].
The factors that contribute to the development of infections at surgical sites can be divided into patient-related or procedure-related variables, among others. Other risk factors involve the indications for surgery, the volume of surgeries performed at each department, the working environment in the operation room and the season of the year [1]. Overall, the most popular SSI pathogen reported by the WHO is Staphylococcus aureus (with 30.4%), followed by coagulase-negative staphylococci (11.7%), Escherichia coli (9.4%) and Enterococcus faecalis (5.9%) [1]. An effective measure, antibiotic prophylaxis has recently been recommended for use in the preoperative and postoperative period to reduce the SSI rate [10]. Also, Boxma et al. have emphasized that accurate prophylactic antibiotic use has been integral to orthopedic and trauma surgery practice in the prevention of SSIs [11]. However, the use of antibiotic prophylaxis is generally low in Vietnam and there are many barriers in applying guidelines for prophylaxis in clinical practice. Hence, developing and implementing prophylactic antibiotics programs integrated into management strategies for overall antibiotic use is essential to secure improvement in the quality of antibiotic use in hospital surgical departments [12, 13]. The current study was carried at Nguyen Dinh Chieu Hospital, which is the largest general hospital located in Ben Tre province, Vietnam, with more than 1000 beds [14]. Although patients with surgery account for a considerable number of hospital admissions, there is still little evidence regarding the use of antibiotic prophylaxis at this hospital. As a result, our study was designed to investigate trends in using antibiotic prophylaxis for SSI prevention at Nguyen Dinh Chieu Hospital, Vietnam.
METHODS
Study Design
A retrospective study was conducted by obtaining the medical records of patients who underwent surgical procedures at Nguyen Dinh Chieu Hospital, Ben Tre province from January to September 2019.
Data Collection
The medical records included in our study were of patients aged between 16 and 66, who had undergone surgery and received prophylactic antibiotics. Exclusion criteria involved inaccessible records or insufficient data for the descriptive analysis. We excluded surgical patients who did not receive prophylactic antibiotics and those who discharged themselves or were transferred to another hospital. Patients who were admitted to the surgical emergency unit were also excluded from the study. There were 5245 medical records at the hospital during the study period but only 407 records that met the criteria were included in the analysis. The process of selecting the study sample is shown in Figure 1.
Figure 1. Sample size determination
Data were obtained on socio-demographic characteristics and clinical aspects of the patient as well as trends in using surgical antibiotic prophylaxis at the hospital. Information about socio-demographic characteristics comprised age, age group, and gender, while clinical characteristics were collected about co-morbidities, duration of surgical operations, length of hospital stay, length of preoperative hospital stay, length of postoperative hospital stay, wound classification, type of infection and other facets related to the infection. Concerning surgical prophylactic antibiotics, we recorded prescribed antibiotics, the antibiotic regime, the route of administration, and the timing of both preoperative and postoperative antibiotic prophylaxis.
Statistical Analysis
Data were entered into Microsoft Excel 2016 and then cleaned before exporting to Statistical Package for the Social Sciences (SPSS) version 20.0 for further management and analysis. Descriptive statistical methods were used to present socio-demographic aspects of patients as well as trends in antibiotic prophylaxis. In particular, frequency and percentage were calculated to describe categorical variables, whereas mean, median and interquartile ranges (IQR) were used to summarize continuous variables.
Ethical Approval
The research protocol was approved for implementation by the Ethics Council of the Hospital. All participants agreed to be enrolled in the study. Personal information was kept confidential and the data collected were used only for research purposes. Some sensitive information was encrypted to avoid disclosing participants' data.
RESULTS
A total of 407 surgical records at the hospital were included in this study. The average age of patients was 35.2±14.4 years and more than half (55.1%) were aged between 21 and 40, followed by 29.8% patients in the 41–60 age group. The proportion of female patients was 60.7%, which was 1.5 times higher than the figure for male patients (39.3%) (Table 1).
|
Table 1. Socio-demographic characteristics of patients undergoing surgery at Nguyen Dinh Chieu hospital (n=407) |
||
|
Variables |
Frequency (n) |
Percentage (%) |
|
Age (years) |
|
|
|
Mean ± SD |
35.2±14.4 |
|
|
Median (Q1 - Q3) |
33 (27-53) |
|
|
Age groups (years) |
|
|
|
18 - ≤ 20 |
43 |
10.5 |
|
21 - 40 |
225 |
55.3 |
|
41 - 60 |
121 |
29.8 |
|
> 60 |
18 |
4.4 |
|
Gender |
|
|
|
Male |
160 |
39.3 |
|
Female |
247 |
60.7 |
Among the 407 participants, 51 patients had co-morbidities, accounting for 12.4% of the sample. In particular, heart disease had the greatest prevalence among patients (at 4.9%), compared to diabetes and chronic obstructive pulmonary disease (at 1.7% each). Open surgery was used in the majority of procedures (72.2%), and 53.1% were emergencies. The average duration of surgery was about 35 minutes and the median hospitalization duration was 7 days. While patients rarely stay at the hospital before surgery, they generally stay for six days after undergoing an operation. Contaminated wounds (54.8%) were the most common site of SSI, followed by clean-contaminated wounds (31.9%), clean wounds (7.6%) and dirty wounds (5.7%). Three-tenths of procedures were cesarean sections, the most frequent type of surgery performed at the hospital. In this study, 2.5% of patients were diagnosed with bacterial infection and 37.6% had signs of infection before surgery. A white blood cell ratio of more than 10,000/mm3 had the highest percentage of the four clinical signs of infection (76.1%). At the same time, 20 patients had systemic inflammatory response syndrome, accounting for 4.9% of the sample. Regarding SSI, only two patients were diagnosed with superficial incisional SSI, accounting for less than one percent. No patients were found to be infected with other types of SSI including deep incisional SSI, organ/space SSI, or remote infection (Table 2).
|
Table 2. Clinical characteristics of patients undergoing surgery at Nguyen Dinh Chieu hospital (n=407) |
||
|
Variables |
Frequency (n) |
Percentage (%) |
|
Co-morbidities |
|
|
|
Heart diseases |
20 |
4.9 |
|
Diabetes |
7 |
1.7 |
|
Chronic Obstructive Pulmonary Disease (COPD) |
7 |
1.7 |
|
Gastrointestinal disorders |
5 |
1.2 |
|
Others |
12 |
2.9 |
|
Methods of surgery |
|
|
|
Open surgery |
294 |
72.2 |
|
Endoscopy surgery |
113 |
27.8 |
|
Surgical procedure |
|
|
|
Elective |
191 |
46.9 |
|
Emergency |
216 |
53.1 |
|
Duration of surgery (minutes) |
|
|
|
Median (Q1 – Q3) |
35 (29-55) |
|
|
Length of hospital stay (days) |
|
|
|
Median (Q1 – Q3) |
7 (5 – 8) |
|
|
Length of preoperative hospital stay (days) |
|
|
|
Median (Q1 – Q3) |
0 (0 – 2) |
|
|
Length of postoperative hospital stay (days) |
|
|
|
Median (Q1 – Q3) |
6 (4 – 7) |
|
|
Wound classification |
|
|
|
Clean |
31 |
7.6 |
|
Clean-contaminated |
130 |
31.9 |
|
Contaminated |
223 |
54.8 |
|
Dirty |
23 |
5.7 |
|
Types of surgery |
|
|
|
Cesarean section |
122 |
30.0 |
|
Orthopedic surgery |
87 |
21.4 |
|
Appendectomy |
68 |
16.7 |
|
Hysterectomy |
43 |
10.6 |
|
Head and neck surgery |
28 |
6.9 |
|
Urological surgery |
20 |
4.9 |
|
Inguinal hernia repair |
15 |
3.7 |
|
Partial colectomy |
12 |
2.9 |
|
Others |
12 |
2.9 |
|
Characteristics of infection |
|
|
|
Confirmed infection |
10 |
2.5 |
|
Symptoms of infection |
153 |
37.6 |
|
White blood cells (WBCs)/ peripheral blood > 10,000/mm3 |
116 |
28.5 |
|
White blood cells (WBCs)/ urine (+) |
62 |
15.2 |
|
Abscess |
33 |
8.1 |
|
Body temperature >38.5oC |
13 |
3.2 |
|
Systemic inflammatory response syndrome |
20 |
4.9 |
|
Surgical site infection |
|
|
|
Superficial incisional SSI |
3 |
0.7 |
|
Deep incisional SSI |
0 |
0.0 |
|
Organ or space SSI |
0 |
0.0 |
|
Remote infection |
0 |
0.0 |
In total, the 407 patients were given 2722 prescriptions for prophylactic surgical antibiotics at the hospital. The most commonly used antibiotic combination of the b-lactam group and b-lactamase inhibitor was Amoxicillin/Sulbactam (at 28.6%), followed by Metronidazole (27.6%). Also, Ceftezole, a first-generation cephalosporin, which is usually recommended in SSI prevention, accounted for 19.1% (Table 3).
|
Table 3. Surgical antibiotic prophylaxis uses at Nguyen Dinh Chieu Hospital |
||
|
Antibiotics |
Frequency (n) |
Percentage (%) |
|
Amoxicillin/sulbactam |
777 |
28.6 |
|
Ceftezole |
520 |
19.1 |
|
Ceftizoxime |
267 |
9.8 |
|
Cefoperazone/sulbactam |
88 |
3.2 |
|
Metronidazole |
752 |
27.6 |
|
Ciprofloxacin |
272 |
10.0 |
|
Moxifloxacin |
5 |
0.2 |
|
Levofloxacin |
24 |
0.9 |
|
Cefuroxime |
17 |
0.6 |
|
Total |
2,722 |
100.0 |
The most commonly chosen prophylactic antibiotics for multiple types of surgery were β-lactam/β-lactamase inhibitors (Amoxicillin/Sulbactam) and first-generation cephalosporins (Ceftezole). Third-generation cephalosporins were also prescribed for surgical patients but only accounted for minor amounts, except for cesarean surgery (29.5%). Also, other antibiotics used, often in combination with β-lactam antibiotics, were Fluoroquinolone (Ciprofloxacin) or Metronidazole.
Among the different types of surgery, the most frequent antibiotic use was observed in cesarean sections (at 512 doses), with Amoxicillin/Sulbactam (at 70.5%) and Ceftixoxime (at 29.5%). Amoxicillin/Sulbactam and Metronidazole formed the most frequent combination antibiotic therapy used in orthopedic surgery, with over 50%. Combination antibiotic therapy, consisting of cephalosporins with Metronidazole or Ciprofloxacin, was the only antibiotic treatment given to patients who underwent an appendectomy. By contrast, those who underwent head and neck surgery, hysterectomy, urological surgery, or inguinal hernia repair were mainly prescribed single antibiotic therapy (Table 4).
|
Table 4. Surgical antibiotic prophylaxis uses in different types of surgery |
||
|
Frequency (n) |
Percentage (%) |
|
|
Cesarean section |
512 |
100.0 |
|
Amoxicillin/sulbactam |
361 |
70.5 |
|
Ceftizoxime |
151 |
29.5 |
|
Orthopedic surgery |
346 |
100.0 |
|
Amoxicillin/sulbactam; metronidazole |
181 |
52.3 |
|
Ceftizoxime; metronidazole |
76 |
22.0 |
|
Cefoperazone/sulbactam; ciprofloxacin Metronidazole |
58 |
16.8 |
|
Ceftizoxime |
31 |
8.9 |
|
Appendectomy |
269 |
100.0 |
|
Ceftezolee; metronidazole |
181 |
67.3 |
|
Ceftezolee; ciprofloxacin; metronidazole |
71 |
26.4 |
|
Cefoperazone/sulbactam; ciprofloxacin; metronidazole |
17 |
6.3 |
|
Hysterectomy |
160 |
100.0 |
|
Amoxicillin/sulbactam |
88 |
55.0 |
|
Amoxicillin/sulbactam; metronidazole |
67 |
41.9 |
|
Ceftizoxime |
5 |
3.1 |
|
Head and neck surgery |
113 |
100.0 |
|
Amoxicillin/sulbactam |
80 |
70.8 |
|
Ceftezolee |
29 |
25.7 |
|
Ceftizoxime |
4 |
3.5 |
|
Urological surgery |
101 |
100.0 |
|
Ceftezolee; ciprofloxacin |
84 |
83.2 |
|
Levofloxacin |
17 |
16.8 |
|
Inguinal hernia repair |
63 |
100.0 |
|
Ceftezolee |
46 |
73.0 |
|
Ceftezolee; metronidazole |
17 |
27.0 |
|
Partial colectomy |
95 |
100.0 |
|
Ceftezolee; metronidazole |
42 |
44.2 |
|
Ceftezolee; ciprofloxacin; metronidazole |
29 |
30.5 |
|
Cefuroxime |
17 |
17.9 |
|
Levofloxacin (oral) |
7 |
7.4 |
|
Others |
39 |
100.0 |
|
Ceftezolee |
21 |
53.8 |
|
Cefoperazone/sulbactam; ciprofloxacin; metronidazole |
13 |
33.3 |
|
Moxifloxacin |
5 |
12.9 |
The single antibiotic regimen was used for the prevention of SSIs more than combination therapy, with 836 single antibiotic prescriptions (accounting for over 50%). Penicillin (especially Amoxicillin) and β-lactamase inhibitors were used the most frequently (63.3% of all single antibiotics), followed by first-generation cephalosporins (22.8%). The percentage of first and second-generation cephalosporins given to patients was far lower at only 9% and 2%, respectively. Regarding combination antibiotic therapy, 648 prescriptions used double combinations and 175 using triple combinations. Metronidazole was the most common antibiotic prescribed in combination therapy with β-lactam agents. The combination of Metronidazole and Penicillin/β-lactamase inhibitors accounted for 38.3%, whereas combined use with first generation cephalosporins accounted for 37.0%. In addition, double therapy comprising cephalosporins and Metronidazole or cephalosporins and Fluoroquinolone made up approximately the same share at 11.7% and 13.0%, respectively. Concerning triple therapy, more than half (57.1%) of combinations included first generation cephalosporins, Fluoroquinolone and Metronidazole (Table 5).
|
Table 5. Antibiotic regimes used at Nguyen Dinh Chieu hospital |
||
|
Antibiotic regime |
Frequency (n) |
Percentage (%) |
|
Single antibiotic regime |
836 |
100.0 |
|
Penicillin/ β-lactamase inhibitors |
529 |
63.3 |
|
C3G |
191 |
22.8 |
|
C1G |
75 |
9.0 |
|
FQ |
24 |
2.9 |
|
C2G |
17 |
2.0 |
|
Double antibiotic combinations |
648 |
100.0 |
|
C1G + Metronidazole |
240 |
37.0 |
|
Penicillin/ β-lactamase inhibitors + Metronidazole |
248 |
38.3 |
|
C3G + Metronidazole |
76 |
11.7 |
|
C1G + FQ |
84 |
13.0 |
|
Triple antibiotic combinations |
175 |
100.0 |
|
C1G + FQ + Metronidazole |
100 |
57.1 |
|
C3G/ UC β-lactamase + FQ + Metronidazole |
75 |
42.9 |
|
C1G: first-generation cephalosporins C2G: second-generation cephalosporins C3G: third-generation cephalosporins UC β-lactamase: β-lactamase inhibitors FQ: Fluoroquinolones |
||
Table 6 shows the proportion of patients receiving prophylactic antibiotics in terms of dose size and route of administration. Concerning intravenous injection, Amoxicillin combined with Sulbactam at a dose of 500/250 mg had the highest figure, accounting for 19.4%. Also, the percentage of Ceftezole 2000 mg was the second-highest figure at 18.8%. The main antibiotic used for intravenous infusion was Metronidazole (with doses of 500 mg and 1000 mg), and Fluoroquinolones. Two oral antibiotics, Levofloxacin 500 mg and Cefuroxime 500 mg, were used much less, with 0.9% and 0.6%, respectively.
|
Table 6. Route of administration and dosage of surgical antibiotic prophylaxis |
|||
|
Antibiotics |
Dose |
Frequency (n) |
Percentage (%) |
|
Intravenous injection |
1,652 |
60.7 |
|
|
Amoxicillin/sulbactam |
500/250mg |
528 |
19.4 |
|
Amoxicillin/sulbactam |
1000/500mg |
240 |
8.8 |
|
Amoxicillin/sulbactam |
1000/500mg |
9 |
0.3 |
|
Ceftezolee |
2000mg |
511 |
18.8 |
|
Ceftezolee |
500mg |
9 |
0.3 |
|
Ceftizoxime |
1000mg |
267 |
9.8 |
|
Cefoperazon/sulbactam |
1000/1000mg |
88 |
3.3 |
|
Intravenous infusion |
1,029 |
37.8 |
|
|
Metronidazole |
500mg |
686 |
25.2 |
|
Metronidazole |
1000mg |
66 |
2.4 |
|
Ciprofloxacin |
200mg |
235 |
8.6 |
|
Ciprofloxacin |
400mg |
37 |
1.4 |
|
Moxifloxacin |
400mg |
5 |
0.2 |
|
Oral administration |
41 |
1.5 |
|
|
Levofloxacin |
500mg |
24 |
0.9 |
|
Cefuroxime |
500mg |
17 |
0.6 |
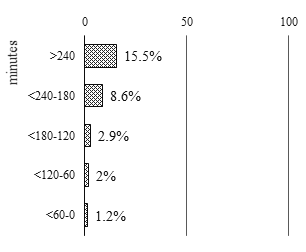
The proportion of patients who used antibiotics before surgical incision and after surgery according to the time of first use are depicted in Figure 2. Of these, 15.5% used antibiotics for over 240 minutes before surgical incision and the corresponding figure decreased gradually, following a shorter time interval, to 1.2% for less than an hour. The opposite trend was observed in the percentage of patients after surgery. While 66.1% of patients were given antibiotics for less than 60 minutes, 1.6% used antibiotics for between 180 and 240 minutes after the operation (Figure 2).
Preoperative
Postoperative

Figure 2. Timing of preoperative and postoperative antibiotic prophylaxis
DISCUSSION
Clinical Characteristics of Patients with Surgery at Nguyen Dinh Chieu Hospital
There were 51 patients in the study with co-morbidities, the most common of which were cardiovascular disease and diabetes. High blood glucose levels in people with diabetes has the potential to lead to the occurrence of SSIs. Also, in a systematic review, Martin et al. (2016), have concluded that diabetes is an independent risk factor for SSIs across multiple types of surgical procedure [15]. Many studies have argued that the duration of surgery is a risk factor for SSIs in various types of surgery. Patients with SSIs often underwent a surgery duration of more than 30 minutes longer than those without SSIs [16, 17]. In our study, the median surgical duration was 35 minutes.
The length of preoperative hospital stays also played a role in the risk of SSI among patients. The longer the length of preoperative stay, the more micro-organisms the patient was exposed to, especially antibiotic-resistant bacteria in the hospital. Our findings show that more than 50% of patients in this study underwent emergency surgery (surgery on the day of admission). According to surgery classification based on the risk of surgical infection of Altemeier, the risk of SSI in patients with contaminated wounds was from 10 to 15% compared to those with dirty wounds, with the risk increasing to more than 25% [18]. Data from the present study were based on the information from surgical records at Nguyen Dinh Chieu hospital, with the percentage of contaminated and dirty wounds accounting for over 60%. However, a classification of surgery based on the risk of SSIs has not been routinely conducted by surgeons at the hospital. Due to a large proportion of SSIs, appropriate risk assessment and classification is needed to implement preventive strategies to ensure the safety of patients.
There was a variety of types of surgery in our study. Hysterectomy, appendectomy, orthopedic surgery and cesarean sections made up over 10% of total surgical cases. Patients undergoing these types of surgery were admitted to General Surgery departments, the Department of Orthopedic Surgery and the Department of Obstetrics, which are the main departments where patients are assigned to have surgery at the hospital. Patients with infections before surgery, especially at surgical sites, were at a higher risk of two SSIs in comparison with those without infections. In the present study, 2.5% of patients were diagnosed with an infection before surgery and 37.6% had symptoms of infection. Also, 4.9% of patients with systemic inflammatory response syndrome would be at a high risk of sepsis or septic shock.
Trends in Using Surgical Antibiotic Prophylaxis at Nguyen Dinh Chieu Hospital
- Surgical prophylactic antibiotic therapy
In this study, the rate of using a single antibiotic regimen or a combination antibiotic regimen was nearly equal, accounting for 50.4% and 49.6%, respectively. Specifically, 31.4% of patients undergoing an appendectomy, head and neck surgery, urological surgery and partial colectomy were prescribed single antibiotics, which is contrary to the recommendations of the American Society of Health-System Pharmacists (ASHP) to use combination antibiotics. The high proportion of patients using combination antibiotic regimens may also be due to a large number of patients with dirty and contaminated surgeries in the sample. Also, common prophylactic antibiotics used for SSI prevention comprised Amoxicillin/Sulbactam (28.5%), Metronidazole (27.6%), Ceftezole (19.1%), Ciprofloxacin (10.0%), and Ceftixoxime (9.8%). Our results were not consistent with the recommendations from ASHP (2013) [19]. Amoxicillin/Sulbactam was the most frequently used prophylactic for treatment at the hospital but it is not included in the recommendations of ASHP (2013) [19]. Also, we did not find any guidelines that recommended giving Amoxicillin/Sulbactam to patients for the prevention of SSIs. Therefore, we think that treatment with Amoxicillin/Sulbactam in this situation should be closely examined. According to ASHP, Metronidazole should be used in surgery where patients may be at risk of anaerobic infections such as biliary surgery, laparoscopy, appendectomy, partial colectomy, clean-contaminated head and neck surgery, and urological surgery [19]. In the present study, the treatment of orthopedic surgery patients with Metronidazole may not be really necessary as this antibiotic is not included in the ASHP (2013) guideline. First-generation and second-generation cephalosporins are often recommended as surgical antibiotic prophylaxis for SSIs. Although the prescription of Cefuroxime is recommended, only 0.6% of patients were given the antibiotic. By contrast, the percentage of patients used Ceftezole was 19.1% despite the antibiotic not being recommended by ASHP. Concerning ASHP (2013), Fluoroquinolones are indicated when patients are allergic to b-lactam antibiotics, but there was no case of b -lactam allergy in this sample [16]. However, Fluoroquinolones potentially increase the rate of Escherichia coli resistance and the risk of severe adverse effects like tendonitis and tendon rupture. Thus, only one dose of Fluoroquinolones should be given before surgery, whereas all the patients who were taking Fluoroquinolones in our study received many doses of the drug [16, 19].
- Routes of Administration
For most types of surgery, prophylactic antibiotics are usually recommended via intravenous injection because drugs are absorbed quickly and reach a high concentration in the blood at the surgical site. This route is predictable and less likely to be affected by risk factors than the oral route [19]. Our results supported these statements with the majority of patients being given antibiotic prophylaxis via intravenous injection. Intravenous infusion and oral routes were also used at the hospital, accounting for 37.8% and 1.5%, respectively. Oral antibiotics have been evaluated for their effectiveness, and are recommended only for partial colectomy [19]. Our findings show that oral antibiotics were given to a few patients with partial colectomy
- Dosage of Antibiotics
To reduce the incidence of SSIs, prophylactic antibiotics should be used at appropriate doses so that antibiotic concentrations in blood and tissue are sufficient to inhibit bacteria at the incision site and so prevent infection [20]. The dosage of prophylactic antibiotics is usually equivalent to the maximum single dose of the antibiotic. In our study, the majority of prophylactic antibiotics were prescribed at the usual dose and the dose did not vary between the preoperative and postoperative periods. In some cases, however, lower doses were used, namely, Ciprofloxacin intravenous infusion at 200 mg in 235 patients (8.6%) or Amoxicillin/Sulbactam at 500/250 mg via intravenous injection in 528 patients (19.4%), whereas only 66 patients (2.4%) were given higher doses than usual (intravenous infusion of Metronidazole 1000 mg). The use of prophylactic antibiotics at lower doses than recommended may not be effective in preventing SSIs.
- Timing of Preoperative Antibiotic Prophylaxis
The timing of the first dose of antibiotic prophylaxis plays a vital role in the effectiveness of antibiotics for SSI prevention among patients with surgery. Inappropriate timing of administration fails to ensure sufficient drug concentrations in the blood to inhibit bacteria at the surgical site during the procedure [19]. Concerning a systematic review, the administration of antibiotic prophylaxis more than 120 minutes before an incision is associated with a higher risk of SSIs compared to their administration less than 120 minutes before incision [21]. WHO also recommends that antibiotic prophylaxis should be administrated less than 120 minutes before incision [1]. In our study, only 3.2% of patients took prophylactic antibiotics less than 120 minutes before incision and 27% of them received their first dose of antibiotics more than 120 minutes before surgery. This result could lead to a high incidence of SSIs, especially after hospital discharge.
Limitations
Several limitations need to be taken into consideration in the study. First, due to the data of the retrospective study being obtained from medical records at the hospital, some patient characteristics related to the treatment regimen or the prescribed antibiotics have not been investigated. Secondly, the collected data did not include details of the therapy used for the treatment, which may also be the reason for the compulsory use of antibiotic prophylaxis. Thirdly, the findings were not able to evaluate whether or not antibiotics were used appropriately. Also, as the present study was conducted within a short time frame, it cannot generalize for the trend in using prophylactic antibiotics in the southern region or the whole country.
Further research should record more specific patient information to analyze and assess the indication or selection of antibiotics and combination antibiotics. Also, it is necessary to perform microbiological tests, designed to accurately diagnose the cause of disease, in combination with an antibiogram to predict the appropriate antibiotic therapy.
CONCLUSIONS
This retrospective study determined trends in using antibiotic prophylaxis to prevent SSI by analyzing medical records at Nguyen Dinh Chieu Hospital. The use of single antibiotic therapy was similar to the figures for combination therapy. However, prophylactic antibiotics given to patients undergoing surgery at the hospital were unlikely to follow the recommendations of clinical practice guidelines. Most antibiotics were administrated by intravenous infusion because of the rapid response. While the majority of prophylactic antibiotics were prescribed at the usual dose, some antibiotics were used at lower doses than usual making the reduction of SSIs less likely. Hence, strict implementation of guidelines for the prevention of the infection should be ensured among all surgical cases at the hospital.
ACKNOWLEDGEMENTS
The authors would like to express their deep sense of gratitude to the Nguyen Dinh Chieu Hospital for its support for the implementation of this study. They also would like to acknowledge the contribution of the data collators and the patients who voluntarily enrolled themselves in the study.
Conflicts of interest
The authors declare no potential conflicts of interest.
REFERENCES
- World Health Organization. Global guidelines for the prevention of surgical site infection. World Health Organization; 2016.
- Evrilia SR, Muhtadi A, Barliana MI, Winarni R. An evaluation of Ceftriaxone use in the antimicrobial stewardship program for surgical patients at a Hospital in Bandung. Journal of Advanced Pharmacy Education & Research| Jan-Mar. 2019;9(1).
- Boyle KK, Rachala S, Nodzo SR. Centers for disease control and prevention 2017 guidelines for prevention of surgical site infections: review and relevant recommendations. Current reviews in musculoskeletal medicine. 2018 Sep 1;11(3):357-69.
- Allegranzi B, Bischoff P, de Jonge S, Kubilay NZ, Zayed B, Gomes SM, Abbas M, Atema JJ, Gans S, van Rijen M, Boermeester MA. New WHO recommendations on preoperative measures for surgical site infection prevention: an evidence-based global perspective. The Lancet Infectious Diseases. 2016 Dec 1;16(12):e276-87.
- Mawalla B, Mshana SE, Chalya PL, Imirzalioglu C, Mahalu W. Predictors of surgical site infections among patients undergoing major surgery at Bugando Medical Centre in Northwestern Tanzania. BMC surgery. 2011 Dec;11(1):21.
- Mu Y, Edwards JR, Horan TC, Berrios-Torres SI, Fridkin SK. Improving risk-adjusted measures of surgical site infection for the National Healthcare Safely Network. Infection Control & Hospital Epidemiology. 2011 Oct;32(10):970-8
- Ling ML, Apisarnthanarak A, Madriaga G. The burden of healthcare-associated infections in Southeast Asia: a systematic literature review and meta-analysis. Clinical Infectious Diseases. 2015 Jun 1;60(11):1690-9.
- Zimlichman E, Henderson D, Tamir O, Franz C, Song P, Yamin CK, Keohane C, Denham CR, Bates DW. Health care–associated infections: a meta-analysis of costs and financial impact on the US health care system. JAMA internal medicine. 2013 Dec 9;173(22):2039-46.
- De Lissovoy G, Fraeman K, Hutchins V, Murphy D, Song D, Vaughn BB. Surgical site infection: incidence and impact on hospital utilization and treatment costs. American journal of infection control. 2009 Jun 1;37(5):387-97.
- Warnock M, Ogonda L, Yew P, McIlvenny G. Antibiotic Prophylaxis Protocols and Surgical Site Infection Rates in Trauma Surgery: A Prospective Regional Study of 26,849 Procedures. The Ulster medical journal. 2019 May;88(2):111-4.
- Boxma H, Broekhuizen T, Patka P, Oosting H. Randomised controlled trial of single-dose antibiotic prophylaxis in surgical treatment of closed fractures: the Dutch Trauma Trial. The Lancet. 1996 Apr 27;347(9009):1133-7.
- AlOsaimi KM, Kambal AM, AlOtaibi FM, AL-Anazi AB, AlMotairi AR, AlGhamdi WM, Altujjar AR. Factors Affecting Physicians' Choice of Antibiotics for Treatment of Community Acquired Urinary Tract Infections and Their Correlation with Antimicrobial Susceptibility Test Results in King Khalid University Hospital during 2013-2014. International Journal of Pharmaceutical Research & Allied Sciences. 2018 Jan 1;7(1).
- Bhandari MA, Vats N. ANTIBIOTIC PROPHYLAXIS FOLLOWING SIMPLE EXODONTIA: A CONTROLLED TRIAL. Annals of Dental Specialty Vol. 2019 Jan;7(1):1.
- Nguyen Dinh Chieu Hospital, Introduction, Nguyen Dinh Chieu Hospital, [Online]. Available at http://bvndc.vn/lich-su-hinh-thanh. [Accessed: 05/10/2019].
- Martin ET, Kaye KS, Knott C, Nguyen H, Santarossa M, Evans R, Bertran E, Jaber L. Diabetes and risk of surgical site infection: a systematic review and meta-analysis. infection control & hospital epidemiology. 2016 Jan;37(1):88-99.
- Koigi-Kamau R, Kabare LW, Wanyoike-Gichuhi J. Incidence of wound infection after caesarean delivery in a district hospital in central Kenya. East African medical journal. 2005 Jul;82(7):357-61.
- Cheng H, Chen BP, Soleas IM, Ferko NC, Cameron CG, Hinoul P. Prolonged operative duration increases risk of surgical site infections: a systematic review. Surgical infections. 2017 Aug 1;18(6):722-35.
- Altemeier A. Definitions and classifications of surgical infections. Manual on control of infection in surgical patients. 1984;1:19-30.
- Bratzler DW, Dellinger EP, Olsen KM, Perl TM, Auwaerter PG, Bolon MK, Fish DN, Napolitano LM, Sawyer RG, Slain D, Steinberg JP. Clinical practice guidelines for antimicrobial prophylaxis in surgery. Surgical infections. 2013 Feb 1;14(1):73-156.
- Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR, Hospital Infection Control Practices Advisory Committee. Guideline for prevention of surgical site infection, 1999. Infection Control & Hospital Epidemiology. 1999 Apr;20(4):247-80.
- de Jonge SW, Gans SL, Atema JJ, Solomkin JS, Dellinger PE, Boermeester MA. Timing of preoperative antibiotic prophylaxis in 54,552 patients and the risk of surgical site infection: A systematic review and meta-analysis. Medicine. 2017 Jul;96(29):e6903.
