Archive \ Volume.11 2020 Issue 2
Effect of virtual reality training on post-menopausal osteoporotic women
Gopal Nambi1*, Walid Kamal Abdelbasset1,2, Samah Alsaid Moawd1,3, Hend Reda Sakr4, Tamer Emam Elnegamy1, Julie Saji George1
1 Department of Physical Therapy and Health Rehabilitation, College of Applied Medical Sciences, Prince Sattam bin Abdulaziz University, Alkharj, Saudi Arabia.2 Department of Physical Therapy, Kasr Al-Aini Hospital, Cairo University, Giza, Egypt.3 Department of Physical Therapy for Cardiovascular/Respiratory Disorder and Geriatrics, Faculty of Physical Therapy, Cairo University, Giza, Egypt.4 Department of Physical Therapy for Gynecology and Obstetrics, Faculty of Physical Therapy, Badr University, Cairo, Egypt.

Abstract
Generally, virtual reality training (VRT) has been used for the neurosomatic patients to treat the balance problems. The practical application about the effective implementation of this training in osteoporotic post-menopausal women is lacking in medical field. The aim of this study is to find the effects of virtual reality training in bone mineral density, bone mineral content and the quality of life in osteoporotic post-menopausal women. This is a study with an experimental design. 45 participants were equally divided into virtual reality training group VRT-G (n=15), multi-exercise training group MET-G (n=15) and control (n=15) group and undergone 12 weeks of training program. Bone mineral density, bone mineral content and the quality of life were measured before and after 12 weeks of training program. After the training, VRT group shows more significant changes in bone mineral density and bone mineral content than the other two groups (p<0.05). Quality of life measures such as pain, activities of daily living, jobs around the house, mobility, leisure & social activities, general health perception and mental function also showed more improvement in VRT group than the other two groups (p<0.05). The study reported that virtual reality training has wide beneficial effects on bone mineral density, bone mineral content and quality of effect in post-menopause osteoporotic women which may also reduce the risk of osteoporotic fracture.
Keywords: Virtual reality training; bone mineral density; bone mineral content; quality of life; post-menopause

INTRODUCTION
Osteoporosis is a substantial health and clinical problem with an increased risk for bone fractures which may further lead to pain and functional disability. Medical reports say that females are affected more than males and the prevalence rate is increasing considerably after menopause.[1] It is noted that 30% of post-menopausal women have been suffering from osteoporosis, and 40% of these women will get osteoporotic fractures in near future.[2] The risk for the further fracture increases in double after initial fractures within a period of 6 to 12 months.[3] Moreover, in a study, one third of hip fracture due to osteoporosis was dead in twelve months and the rest of two third were handicapped requiring medical assistance throughout the life.[4]
Medical treatment considering drugs plays an important role in improving the bone mineral density (BMD) and bone mineral content (BMC) in osteoporosis. It significantly reduces the consequences of osteoporosis around 20 – 60% which depends on the selection of drug and its application in patients’ population.[5] It is critically observed that drugs do not have a direct role on the key risk factors for fractures such as muscle strength, muscle power, endurance and overall performance.[6] Training the patient through different forms of exercises is the only approach which strengthens and recovers the muscle properties and reduces the risk factors of osteoporosis. Different types of exercise and exercise guidelines have been prescribed to improve the bone mass and muscle strength for the reduction of risk factors in post-menopausal women.[7] One among the advanced exercise training in the field of physical therapy is virtual reality training.
Generally, virtual reality training (VRT) is used for the neuro somatic patients to treat the balance impairments. The basic concept of VRT is activating the sensory feedback from the patients by means of displaying different virtual games.[8, 9] This type of training has more advantages and benefits than other types of training due to its ease of application. Training through games is more interesting and also safe for the post-menopausal elder women. Numerous studies have given positive outcomes of VRT in neurological conditions through neuroplasticity changes.[10, 11] Hence, this type of training may also have positive effect on reducing the risk factors in osteoporotic post-menopausal women. Therefore, the objective of this study is to find the effects of virtual reality training on bone mineral density, bone mineral content and the quality of life in osteoporotic post-menopausal women.
SUBJECTS AND METHODS
Study Design
This is a study with an experimental design where the participants were equally divided into three groups. 45 post-menopausal women were divided and recruited into three groups such as virtual reality training group VRT-G (n=15), multi-exercise training group MET-G (n=15) and control (n=15) group through non-probability convenience sampling method. The study was approved by the scientific ethical committee with reference no RHPT/019/031 and was conducted according to the ethical guidelines of the declaration of Helsinki 1964 and declaration of Tokyo, 1975. It was executed transparently and presented in accordance with CONSORT guidelines.
An orthopedic surgeon in the university hospital evaluated and referred the eligible participants to the department for the study.
Patient involvement
The detailed information about the study was explained to all the participants by the trained therapist before starting the study. The study information form consists of study design, treatment procedure, research outcome, study period, advantages and disadvantages of the study. Also, the printed form was given to all the participants. All the participants should give the consent to participate in the study after going through the study information form.
Participants
The agreed participants underwent initial evaluation by the orthopedic surgeon to be eligible to be a part in the study. To be included in the study, the participants should have reached menopause three years before. Participants with severe osteoporosis (BMD ≤ 70 g/cm2), having calcium supplementation drugs, involving in any exercise training program and having musculoskeletal, neural and somatic diseases were excluded from the study.
Interventions
The VRT-G, MET-G and Control-G undergone 12 weeks of training program and the pre and post outcome measures were measured. The training program was given and supervised by a trained physiotherapist. The training was specifically given emphasize on strength training of the muscles. The study excluded twelve participants with severe osteoporosis, five with musculoskeletal and soft tissue injuries and eight participants were not given the consent to participate in the study (Figure-1).
The first group (VRT-G group) received the training through the device Pro-Kin system PK 252 N, Italy. Before training all the participants in this group, they were given personal education about virtual reality training which gave clear idea about this training. The training was given in standing position where the participant stands on the virtual platform. This dynamic platform provides the challenge to the participant and the level of difficulty was increased gradually as per performance. The game was shooting game and the participant could perform all the hip and knee movements within her fall limits. Increasing the grades of exercise increases the level of difficulty and also increases the activity of the muscle. The training has to be performed for 45 minutes in a day for 4 days lasting for 12 weeks. [12]
The MET-G group undergone different exercise training protocols such as vertical jumps, aerobic exercise and graded walking. The participants were asked to jump from the height of 5 cm for 10 times and progress to the height of 25 cm. The general aerobic exercise for 30 minutes was carried following vertical jumps. After aerobic exercise, the participants were asked to walk in the range of 50 to 75% heart rate. [13]
The Control-G group was observed without any specific exercise protocol. They were allowed to do their regular activities of daily living. All the participants in the three groups were observed before and after 12 weeks of training.
Dependent Variables
Bone mineral density
The variables of Bone mineral density (BMD) and bone mineral content (BMC) were measured at Lumbar spine (L1 – L4) with the use of dual energy X-ray absorptiometry (DEXA, Siemens, Hamburg, Germany) scan. The participants were placed in supine position and the DEXA scanner was used to measure the variables and it is a reliable and valid method of measuring bone density and content. [13]
Quality of Life
The quality of life of osteoporotic participants was measured with Quality of life questionnaire (International osteoporosis foundation). The questionnaire consists of different domains such as pain, activities of daily living, jobs around the house, mobility, leisure & social activities, general health perception and mental function. All the answers were standardized in 1 to 5 Likert scale in which ‘1’ represents the best and ‘5’ represents the poor quality of life. [7]
Blinding
The participants and the evaluating therapist were blinded throughout the study. Also, the participants were instructed not to disclose their treatment program with the fellow participants to maintain the blinding procedure.
Statistical analysis
All participants’ baseline demographic values were observed and calculated through Levene's test, which describes the homogenous sample selection. The collected pre and post training data were formulated and presented in mean and standard deviation format. One way ANOVA was used to find the difference between and within the groups. The significance level was set at p< 0.05 and the software SPSS software (version 20.0) SPSS Inc, Chicago, Illinois, USA was used.
RESULTS
Participants
All the participants in the three groups completed all the treatment sessions with 100% compliance. The basic characters such as age, height, weight and body mass index did not show any statistical difference between the groups (p≥0.05). The participant’s VO2peak (mL/kg/min) and heart rate (beats/min) were also measured to find the exercise ability to be included in the treatment session. These clinical variables also showed no difference between the three groups (p≥0.05). The demographic and exercise ability variables are shown in Table 1.
BMD and BMC Analysis
The bone pre and post parameters such as BMD and BMC are presented as mean and SD. The pre-treatment scores on BMD and BMC between the VRT-G, MET-G, and Control-G groups showed no significant difference (p≥0.05) which indicates the homogenous population. Twelve weeks of different types of training did not show any statistical difference in BMD (p≥0.05), but it showed considerable statistical difference in BMC (p≤0.05) which is shown in Table 2. An improvement was observed in BMD and BMC more in VRT-G than other two groups (Figures 2 & 3).
Quality of life analysis
The quality of life was analyzed in various domains such as pain, activities of daily living, jobs around the house, mobility, leisure & social activities, general health perception and mental function. Almost all the domains in the quality of life questionnaire pre-treatment scores did not show any statistical significant difference (p≥0.05) between the groups. The post-treatment scores in all the domains showed significant difference (p≤0.001) between the groups. Overall, post hoc analysis on the quality of life showed more tendencies in improvement towards VRT-G group than the other two groups. (Table 3 & Figure 4).
DISCUSSION
Our study observed and found the changes in BMD and BMC parameters in post-menopausal osteoporotic women after virtual reality training and multiple exercise training. These bone parameters were measured through DEXA scan which is a reliable and valid tool to measure the same. Before training, there was a marked reduction in the bone density and bone content in the post-menopausal osteoporotic women, this was in agreement with Cumming et al. [14] Reduction in bone mineral density and content leads to physical incapacity and high risk factor for bone fractures.
In accordance with the reports presented by our study, there was a significant improvement in the increase of BMD and BMC in lumbar spine in VRT group than the other two groups. It generally stimulated the sensory system and fastens the activity of the motor system. This forward feedback system enhanced the power and strength of the particular group of muscles, which provided the weight bearing load on the concerned bones. Based on the real time information form, the participants can progress to the next level and further increase the difficulty level. [15] The improvement in the MET group may be due to different exercise training protocols, and the decrease in the treatment outcomes may be due to the fact that these exercises were under the control of treating therapist. The action behind little changes in the MET group is by the overall improvement of muscle strength and power. [16]
This study also observed the quality of life changes in post-menopausal osteoporotic women after virtual reality training and multiple exercise training. The report showed that VRT training improved the quality of life than the other two groups. VRT improved the quality of life in post-menopausal osteoporotic women by improving changes in pain, activities of daily living, jobs around the house, mobility, leisure & social activities, general health perception and mental function domains.[17] The changes in these domains in VRT were due to the presence of real time games which enhanced the experience related brain plasticity by providing different game experiences. Theses graded exercise program also improved the attention, concentration and memory of these subjects and improved the overall quality of life [18] in VRT group.
The greater strength of this study is analysis of bone mineral density and bone mineral content in post-menopause osteoporosis women after virtual reality training for the first time. However, few limitations were observed throughout the study. First, the sample was small and the second one the long term effects of this training was not analysed.
CONCLUSION
According to the results, virtual reality training has wide beneficial effects on bone mineral density, bone mineral content and quality of effect in post-menopause osteoporotic women which may further reduce the risk of osteoporotic fracture. Future researches are recommended to find the association between the bone mineral density and quality of life in post-menopause osteoporotic women.
ACKNOWLEDGEMENT
The publication was supported by the Deanship of Scientific Research at Prince Sattam bin Abdulaziz University.
REFERENCES
- Wright NC, Looker AC, Saag KG, et al. The recent prevalence of osteoporosis and low bone mass in the United States based on bone mineral density at the femoral neck or lumbar spine. J Bone Miner Res 2014; 29(11):2520-2526.
- Reginster JY, Burlet N. Osteoporosis: a still increasing prevalence, Bone 2006; 38(2 Suppl 1):S4-S9.
- Bliuc D, Alarkawi D, Nguyen TV, Eisman JA, Center JR. Risk of subsequent fractures and mortality in elderly women and men with fragility fractures with and without osteoporotic bonedensity: the Dubbo Osteoporosis Epidemiology Study. J Bone Miner Res 2015; 30(4):637-646.
- Cooper C, Atkinson EJ, Jacobsen SJ, O’Fallon WM, Melton L. 3rd.Population-based study of survival after osteoporotic fractures. Am J Epidemiol 1993; 137(9):1001-1005.
- Crandall CJ, Newberry SJ, Diamant A, et al. Comparative effectiveness of pharmacologic treatments to prevent fractures: an updated systematic review. Ann Intern Med. 2014; 161(10):711-723.
- Cawthon PM, Fullman RL, Marshall L, et al. Osteoporotic Fractures in Men Research G Physical performance and risk of hip fractures in older men. J Bone Miner Res 2008; 23(7):1037-1044.
- Robin M. Dalya, Jack DallaViaa, et al. Exercise for the prevention of osteoporosis in postmenopausal women: an evidence-based guide to the optimal prescription. Brazilian Journal of Physical Therapy 2019; 23(2):170-180.
- Gil-Gomez JA, Llorens R, Alcaniz M, et al. Effectiveness of a Wii balance board-based system (eBaViR) for balance rehabilitation: a pilot randomized clinical trial in patients with acquired brain injury. J Neuroeng Rehabil 2011; 8:30.
- Lange BS, Requejo P, Flynn SM, et al. The potential of virtual reality and gaming to assist successful aging with disability. Phys Med Rehabil Clin N Am 2010; 21(2):339-56.
- Mao Y, Chen P, Li L, et al. Virtual reality training improves balance function. Neural Regen Res 2014; 9(17):1628-34.
- Yesilyaprak SS, Yildirim MS, Tomruk M, et al. Comparison of the effects of virtual reality-based balance exercises and conventional exercises on balance and fall risk in older adults living in nursing homes in Turkey. Physiother Theory Practice 2016; 32(3):191-201.
- Sam-yeol Wi, Jong-ho Kang. The Effects of Virtual Reality Interactive Games on the Balance Ability of Elderly Women with Knee Osteoarthritis. Journal of physics 2012; 7(3):387-393.
- Elena Marín-Cascales, Jacobo Á. Rubio-Arias, Pedro E. Alcaraz. Effects of Two Different Neuromuscular Training Protocols on Regional Bone Mass in Postmenopausal Women: A Randomized Controlled Trial. Frontiers in physiology 2019; 10:846.1-9.
- Cummings S. R, Melton L. J. Epidemiology and outcomes of osteoporotic fractures. Lancet 2002; 359:1761-1767.
- Mao Y, Chen P, Li L, et al. Virtual reality training improves balance function. Neural Regen Res 2014; 4(17):1628-34.
- Mori A. Electromyographic activity of selected trunk muscles during stabilization exercises using a gym ball. Electromyogr Clin Neurophysiol 2004; 44:57-64.
- Ma Y, Wu X, Xiao X, et al. Effects of teriparatide versus percutaneous vertebroplasty on pain relief, quality of life and cost-effectiveness in postmenopausal females with acute osteoporotic vertebral compression fracture: A prospective cohort study. Bone 2019;13;131:115154.
- D’hooge R, Cagnie B, Crombez G, et al. Increased intramuscular fatty infiltration without differences in lumbar muscle cross sectional area during remission of unilateral recurrent low back pain. Man Ther 2012; 12:584-8.
|
Table 1: Demographic characteristics of the participants in VRT, MET and Control groups |
|||||
|
No |
Variable |
VRT – G |
MET – G |
Control – G |
P |
|
1 |
Age (y) |
56.3 ± 2.5 |
57.6 ± 2.7 |
56.5 ± 2.5 |
0.419 |
|
2 |
Height (m) |
1.62 ± 0.16 |
1.64 ± 0.17 |
1.63 ± 0.13 |
0.950 |
|
3 |
Weight (kg) |
68.3 ± 1.5 |
69.6 ± 1.5 |
68.7 ± 1.5 |
0.109 |
|
4 |
BMI (kg/m2 ) |
24.2 ± 1.3 |
24.3 ± 1.5 |
23.9 ± 1.4 |
0.769 |
|
5 |
VO2peak |
37.2 ± 4.5 |
37.5 ± 4.3 |
37.6 ± 4.8 |
0.975 |
|
6 |
HR |
172 ± 5.8 |
171 ± 6.2 |
170 ± 6.2 |
0.724 |
|
Table 2: BMD and BMC analysis of VRT, MET and Control groups |
||||||
|
No |
Variable |
|
VRT – G |
MET – G |
Cont. – G |
P |
|
1 |
BMD (g/cm2) |
Pre |
0.95 ± 0.12 |
0.94 ± 0.15 |
0.97 ± 0.13 |
0.856 |
|
|
|
Post |
1.03 ± 0.13 |
0.98 ± 0.14 |
0.96 ± 0.12 |
0.408 |
|
2 |
BMC (g) |
Pre |
56.48 ± 4.82 |
55.27 ± 5.25 |
57.52 ± 6.11 |
0.598 |
|
|
|
Post |
63.61 ± 4.62 |
59.42 ± 4.54 |
56.72 ± 4.58 |
0.003 |
|
Table 3: Quality of life analysis of VRT, MET and Control groups |
||||||
|
No |
Variable |
Time |
VRT – G |
MET – G |
Control |
P |
|
1 |
Pain |
Pre |
3.28 ± 0.5 |
3.45 ± 0.4 |
3.49 ± 0.5 |
0.514 |
|
|
|
Post |
1.45 ± 0.3 |
2.88 ± 0.2 |
3.28 ± 0.4 |
0.001 |
|
2 |
Activities |
Pre |
4.21 ± 0.3 |
3.93 ± 0.2 |
4.21 ± 0.4 |
0.051 |
|
|
|
Post |
1.28 ± 0.3 |
2.89 ± 0.4 |
4.18 ± 0.3 |
0.001 |
|
3 |
Jobs in the house |
Pre |
3.82 ± 0.3 |
3.62 ± 0.4 |
3.78 ± 0.3 |
0.318 |
|
|
|
Post |
0.18 ± 0.2 |
1.13 ± 0.4 |
3.22 ± 0.3 |
0.001 |
|
4 |
Mobility |
Pre |
4.23 ± 0.3 |
4.54 ± 0.4 |
4.28 ± 0.5 |
0.152 |
|
|
|
Post |
1.21 ± 0.3 |
3.21 ± 0.4 |
3.25 ± 0.4 |
0.000 |
|
5 |
Leisure & social |
Pre |
3.25 ± 0.6 |
2.84 ± 0.5 |
3.25 ± 0.6 |
0.141 |
|
|
|
Post |
0.82 ± 0.4 |
1.65 ± 0.4 |
3.11 ± 0.5 |
0.001 |
|
6 |
General health |
Pre |
4.21 ± 0.4 |
4.34 ± 0.6 |
4.42 ± 0.5 |
0.596 |
|
|
|
Post |
0.64 ± 0.2 |
1.82 ± 0.3 |
4.28 ± 0.4 |
0.001 |
|
7 |
Mental function |
Pre |
03.38± 0.4 |
3.24 ± 0.3 |
3.45 ± 0.4 |
0.377 |
|
|
|
Post |
0.21 ± 0.2 |
1.42 ± 0.3 |
2.75 ± 0.3 |
0.000 |
|
8 |
Quality of Life |
Pre |
3.76 ± 0.4 |
3.70 ± 0.3 |
3.84 ± 0.3 |
0.525 |
|
|
|
Post |
0.82 ± 0.2 |
2.14 ± 0.2 |
3.43 ± 0.3 |
0.001 |
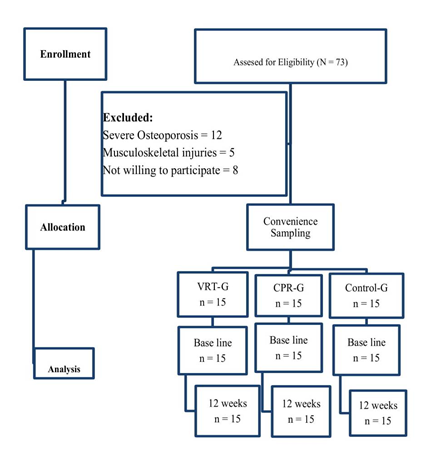
Figure 1: Flow chart showing the study details of VRT, MET and control groups
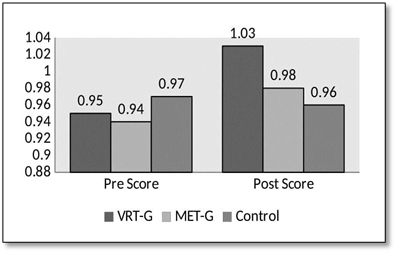
Figure 2: Pre and post scores of Bone mineral density in VRT, MET and control groups
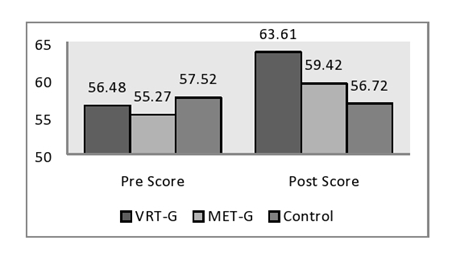
Figure 3: Pre and post scores of Bone mineral content in VRT, MET and control groups
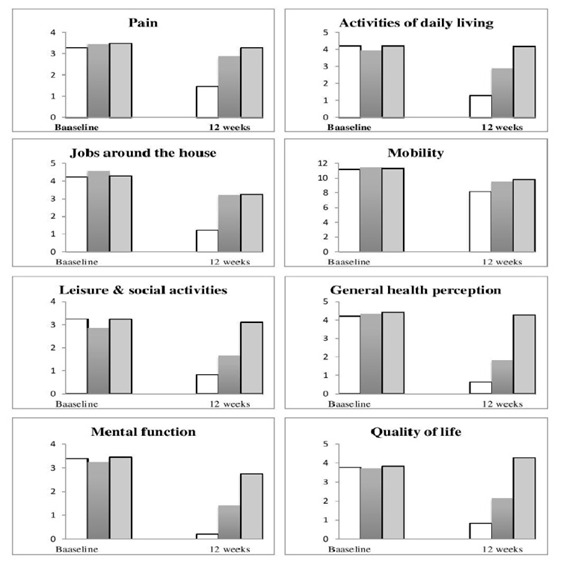
Figure 4: Pre and post scores of various domains of Quality of life in VRT, MET and control groups
