Archive \ Volume.15 2024 Issue 1
Risk Factors in Postpartum Depression Among Women from South-East of Romania: Importance of Early Diagnosis
, , , , , , , ,Abstract
Our research aimed to identify the risk factors that may contribute to postpartum depression (PPD) in the immediate postpartum period. The study was conducted at the University Emergency County Hospital Constanta, Romania, between 2019 and 2021. We included 904 women on the 2nd day of the postpartum period, divided into 2 groups: women with PPD (n=236) and control (women without PPD, n=668). Demographic characteristics and clinical information (i.e., women’s age, urban or rural areas, level of education, Rh blood group, chronic diseases, mode of delivery, women’s parity, and the number of abortions) were assessed. The prevalence of PPD found was 26.1%. Our findings suggest that only the women’s age and level of education were significantly associated with PPD (p=0.05 and p=0.002), being appraised as risk factors in PPD. Our study shows that early detection of PPD represents an important task for its prevention and women should be counseled in order to reduce negative child follow-up.
How to cite:
Download Citation
INTRODUCTION
The changing effects on women’s lives are pregnancy and childbirth. The mother’s availability will decrease in the presence of a newborn, as the baby will become her priority [1]. Postpartum depression (PPD) represents a subtype of major depressive disorders that appear within the 4 weeks after childbirth [2] and can last up to 2 weeks [3]. It is a serious mental illness that involves physical and emotional changes and disturbs approximately 10-20% of mothers widespread [4]. This illness can reveal negative short and long-term features on motherhood and child growth having sometimes disastrous consequences [5-7]. Its frequency varies depending on different diagnostic tools [8-10].
Some studies showed that it depends on psychological stressors [11], and biological factors [12]. Therefore, women with endometriosis and infertility could have had a psychological condition that led them more easily to develop different disorders, like PPD [13]. Until now, its etiology is still not fully understood [14].
Postpartum depressive disorders represent the most often psychiatric conditions observed in women after childbirth, starting from the softer postpartum baby blues to PPD [15]. It emphasized the importance of the identification of depressed women in the immediate postpartum period, as they could develop a major mental disease in the later postpartum period [16, 17].
However, there has been little attention on early PPD among women with high-risk pregnancies such as those who are hospitalized or who suffered great physiological or emotional pressure during pregnancy [18].
By using the Edinburgh postnatal depression scale (EPDS), 14% of American postpartum women were positive for depressive disorders [19]. Reck and contributors [20], reported a rate of 8.7% for depressive disorders measured by EPDS in the first 3 months after birth. Interestingly, the use of EPDS has been shown to increase the detection of women at risk for PPD in comparison with routine clinical tests [21].
Several studies have shown that prenatal depression, self-esteem, prenatal anxiety, marital relationship, infant behavior, socioeconomic status, or unplanned/unwanted pregnancy can be a risk for poor prenatal care [22-24]. Moreover, women with operative or adverse perinatal issues such as cesarean section [25], preterm childbirth [26], or gestational diabetes [27] have also been shown to express more often PPD. Women with a previous history of psychosis or a history of PPD presented also the highest risk for PPD [28, 29].
Nowadays, such studies are scarce worldwide, and we did not find a similar study in our country. More, there is not, up to our knowledge, a report of such a big number of patients, within a relatively short time frame (20 months) or results relative to the Rh blood group. We hypothesized that PPD is more frequent in less educated, younger, women and that it might be influenced by the residence (urban/rural), mode of delivery, parity, number of abortions, chronic diseases, and Rh blood type.
Based on this hypothesis, this study aimed to analyze the role of different risk factors for depression in the immediate postpartum period. Our results could contribute to the early detection and appropriate care of PPD.
MATERIALS AND METHODS
Participants and Data Collection Procedures
We conducted an observational prospective study on immediate postpartum period women who delivered in our Obstetrics & Gynecology Department from a tertiary university hospital. We analyzed the importance of demographic characteristics and clinical information in relation to PPD. All participants were informed regarding the aims and procedures, that the questionnaire was voluntary and confidential, and that they could withdraw from the study at any time. We obtained informed consent from all participants in the study as well as the Agreement of the Ethics Commission (No. 29726/31.05.2021). Between August 2019 and April 2021, we included 904 successive women in the postpartum period, who were divided into 2 groups: women with PPD (n=236) and control (i.e., women without PPD, n=668).
Edinburgh Postnatal Depression Scale (EPDS)
The EPDS was developed by Cox and contributors, for determining the risk for PPD [9]. It consists of a total of 10 questions, each item being scored differently. The lowest possible score is 0, and the highest score is 30. Scores of 0 through 9 indicate mild to moderate PPD, with little intervention required, while scores of 10 or higher suggest PPD, with immediate intervention required [30, 31]. The women were asked to complete the EPDS on the second day (D2) after delivery. The questionnaires were anonymous and took approximately 10-15 min. to fill in. In the cases in which women had difficulty understanding the questions, a nurse read and explained the questions to them, the women answered the questions, and the nurse helped write the responses. We considered the recommended cutoff score of 10 (sensitivity 82%; specificity 86%) [17] to evaluate the level of PPD.
The Demographic Characteristics and Clinical Information
The demographic and clinical features of the women were obtained from electronic records. Women’s age, urban or rural areas, level of education, Rh blood group, chronic diseases (i.e., pregnancy-induced hypertension, gestational diabetes), mode of delivery (vaginal delivery or caesarian section), women’s parity, and the number of abortions were collected.
Criteria for Inclusion and Exclusion
We included 18-45 years old women, without an identified physical or mental abnormality, who delivered a single baby. We excluded women with multiple pregnancies, those who had a psychiatric disorder that required treatment, those with alcohol or drug abuse, or those who couldn’t read or speak our language. All the participants completed the EPDS questionnaire.
Statistical Analysis
Statistical analysis in this study was carried out utilizing IBM SPSS statistics software version 28 as well as Microsoft Excel. The analytical techniques employed included descriptive statistics, visual representations in the form of graphs, and statistical assessments. Data were presented in various formats: mean and standard deviation values for continuous variables. For categorical variables, counts and percentages were used for representation. In terms of hypothesis testing, we employed various tests, namely the Independent Samples Mann-Whitney U test (for non-normally distributed data), Independent Samples T-test, and Chi-Square Test for the comparison of proportions. The choice of the test depended on the nature of the variables under analysis. The level of significance was predetermined at 0.05.
RESULTS AND DISCUSSION
Scores Obtained from the Applied Scales
From the total number of patients (n=904), the presence of PPD was noted in 26.10% (n=236) (Table 1). Of those, seven mothers (2.96%) answered positively (“sometimes”) to the last EPDS question: “The thought of harming myself has occurred to me.” The maximum obtained score was 22. Table 1 presents the scores obtained via the scales that the participants were given.
|
Table 1. Scale scores of patients with and without PPD. |
|||
|
EPDS |
Women with PPD |
Women without PPD |
Mean±SD |
|
N |
% |
||
|
≥10 |
236 |
26.1 |
12.73±2.58 |
|
≤9 |
668 |
73.9 |
4.61±2.85 |
The Analysis of the Demographic Data
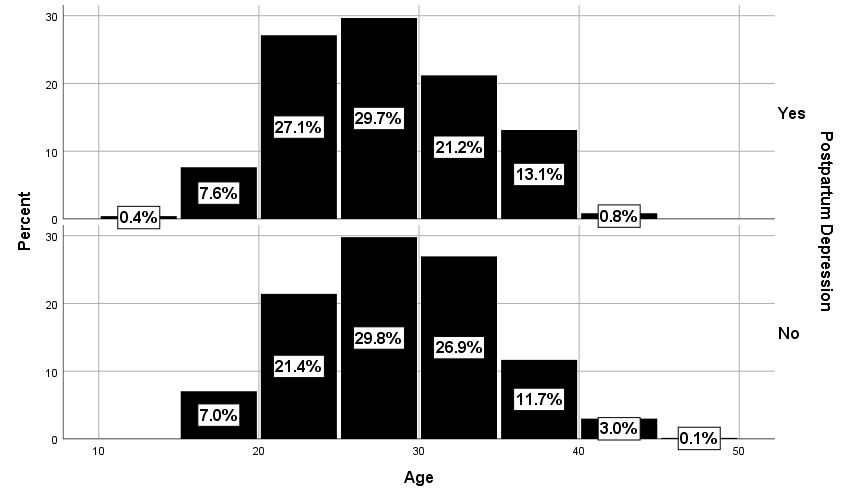
The average age of patients with PPD was 27.34±5.93 (mean±SD) years, and that of those without PPD was 28.23±95.95 years. The difference was statistically significant (Figure 1), (p=0.050), with a younger age being associated with a higher risk of depression.
|
|
|
Figure 1. Age of patients with and without PPD. |
Of the patients with PPD, 51.9% originated from urban areas and 48.1% from rural areas. In the control group (without PPD), 55% originated from an urban environment and 45% from a rural one. Patients with PPD originated from both areas, with almost similar values, and there was no statistical significance between the two groups (Table 2).
|
Table 2. Demographic characteristics of patients with and without PPD. |
|||||
|
Characteristics |
Women with PPD (n=236) |
Women without PPD (n=668) |
P |
||
|
N |
% |
N |
% |
||
|
Area |
|
|
|
|
0.425 |
|
Urban |
120 |
51.9 |
358 |
55 |
|
|
Rural |
111 |
48.1 |
239 |
45 |
|
|
Education |
|
|
|
|
0.002 |
|
4-years |
33 |
14 |
55 |
8.2 |
|
|
8-years |
53 |
22.5 |
113 |
16.9 |
|
|
Professional schools |
1 |
0.4 |
9 |
1.3 |
|
|
High school |
98 |
41.5 |
272 |
40.7 |
|
|
University |
51 |
21.6 |
219 |
32.8 |
|
|
Negative Rh factor |
36 |
15.3 |
74 |
11.1 |
0.093 |
|
Chronic diseases |
26 |
11 |
70 |
10.5 |
0.818 |
|
Mode of delivery |
|
|
|
|
0.818 |
|
Caesarian section |
111 |
47.0 |
320 |
47.9 |
|
|
Vaginal spontaneous |
125 |
53.0 |
348 |
52.1 |
|
|
Pregnancies |
|
|
|
|
0.778 |
|
Primipara |
117 |
49.6 |
320 |
47.9 |
|
|
Secundipara |
69 |
29.2 |
236 |
35.3 |
|
|
Tertipara |
29 |
12.3 |
72 |
10.8 |
|
|
Multipara with > 3 births |
21 |
8.99 |
40 |
5.98 |
|
|
Abortion |
|
|
|
|
0.087 |
|
0 |
138 |
58.5 |
426 |
63.9 |
|
|
1 |
48 |
20.3 |
134 |
20.1 |
|
|
2 |
27 |
11.4 |
63 |
9.4 |
|
|
>2 |
23 |
9.74 |
44 |
6.59 |
|
PPD = postpartum depression.
Among the patients with PPD, 36.9% had primary education (4 years, 8 years, and professional school), and 63.1% had higher education (high school and university) as compared with the group of patients without PPD: 26.4% and 73.5%, respectively (Table 2). The difference was statistically significant (p=0.002). Also, patients with PPD had fewer university studies when compared to patients without PPD (21.6% vs. 32.8%).
The presence of a negative Rh blood group, the history of chronic diseases (i.e., pregnancy-induced hypertension and gestational diabetes), the mode of delivery (vaginal vs. caesarian), and the parity were not statistically significantly correlated with the presence/absence of PPD (Table 2). The same was true for the influence of the number of abortions (Table 2 and Figure 2).
|
|
|
Figure 2. Distribution of patients with and without PPD according to the number of abortions. |

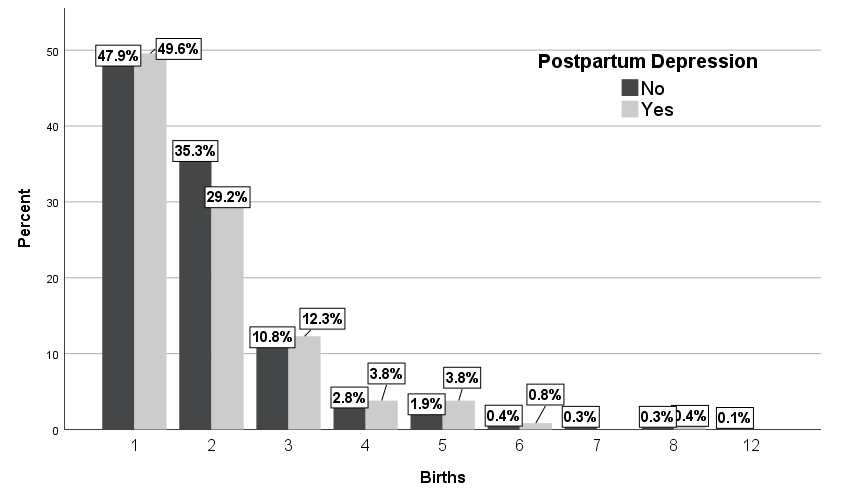
Among the patients with PPD, 49.6% were primipara and 8.89% were multiparous (i.e., more than 3 births). Among the patients without PPD, 47.9% were primipara and 5.98% were multiparous (Table 2 and Figure 3), (p=0.778). These results showed also that primipara women with PPD can be affected more by depression compared with the other categories of parity, but the difference did not reach statistical significance.
|
|
|
Figure 3. Distribution of patients with and without PPD according to the number of births. |
The percentage of women diagnosed with PPD in our study was 26.1%, much higher than the reported for Australia (i.e., 21%), South America (i.e., 19%), Asia (i.e., 16%), North America (i.e., 16%), Africa (i.e., 11%) and Europe (i.e., 8%) [32]. Our study is also in contradiction with Saldanha and contributors [33], where the mean EPDS scores of the depressive population were (statistically significant, p<0.0001) 16.6±2.81, 16.83±3.23 and 15.3±1.87 at 2, 4 and 6 weeks postpartum. In our applied EPDS, the minimum score was 0 and the maximum score was 22, with a cutoff of 10, different from other authors; e.g., Ozturan and contributors used a minimum score of 0, a maximum score of 25, and the cutoff of 13 [34].
There are reports of higher PPD incidence, like the one by Ozturan and contributors [34], 32%, but within a much smaller studied group (124 patients) and from a different region [34]. However, the results of these studies revealed a ratio that ranged between 8 and 26% (i.e., 8% in Europe to 26% in the Middle East), depending on different geographical regions [32].
The mean age of our patients with PPD was 27, with a younger age being associated with a higher risk of depression. This could constitute an explanation of high relevance. Our country is third within the European Union, from the point of view of early maternal age, since 2019 (i.e., 26.9 mean age) [35]. This is in contradiction with the study by Anding and contributors [36], in which the mean age of women with PPD was 40.33 years, without any significant differences. Previous studies have shown no significant association related to age as a risk factor for PPD [37].
Out of the eight elements that we studied, we were able to find a few data in the literature referring to the influence of the urban or rural areas [38] and none about the Rh factor. In our study, of patients with PPD, 51.9% originated from urban areas and 48.1% from rural areas, without any statistical significance. This is in agreement with Zarghami et al. in which PPD predominance was higher among the urban women (20.1%) than that of the rural ones (17.8%) without any significant difference [38]. Another study had similar results, in the prevalence of PPD among women living in rural areas, compared with the ones from a metropolitan zone, without any significant difference [39], which is in contradiction with our study. In the same context, Qi and contributors [40] showed that 41.77% of women with PPD (i.e., EPDS score 10) from 747 lived in urban areas, compared with 38.57% of women with PPD from 70 who lived in rural areas [40].
The level of education was statistically significantly related to PPD occurrence and hence could represent a potential risk factor. These results agree with the study of Saldanha et al. [33] and Yehia et al. in which the level of education was statistically significant in PPD women. Our results are also similar to the results of Naheeda et al. in which mothers with education below 10th standard were more affected by depressive mood (13.8%) when compared to controls (7.5%). However, all these studies included a significantly smaller number of patients: from 186 patients with PPD, 40 (21,5%) had PPD and 146 (78,49%) were without PPD [33]; from 300 patients, only 201 patients (67%) had mild to moderate symptoms of PPD and 48 patients (16%) had high levels of symptoms [41]; from 500 patients, only 8,6% had PPD [42]. Lower levels of education and prenatal counseling (including psychological) as well as younger age, in our groups, could, all, have contributed to this difference.
We could not observe an influence of chronic diseases on PPD occurrence, contrary to some studies that report that pregnancy-related chronic diseases are generally potential risk factors for PPD [43]. Similarly, in our study, the caesarian section as the mode of delivery did not represent a significant feature for PPD, in contradiction with other studies [44]. We also could not find any difference in primipara or multipara women, which is in accordance with the study of Anding and contributors [36]. Another study showed that there was no statistically significant relationship between parity or history of abortion with the onset of PPD [45].
PPD was seen less frequently (but not statistically significant) in patients without any history of pregnancy abortion. Other previous studies have reported a connection between prior miscarriages and PPD [46]. One meta-analysis showed that self-esteem, marital status, socioeconomic status, and unplanned/unwanted pregnancy are new predictors of PPD [47]. Therefore, an EPDS score ≥ 10 on D2 could indicate a PPD and allow us to select the patients who need a closer follow-up during the immediate postpartum period.
Our study included women who gave birth in our hospital, a reference hospital that usually cares for women from all over the country. However, with the lack of national studies assessing the prevalence of PPD in the postnatal period [48, 49], we cannot determine if the age or the education level of women from our study is significantly different from the rest of the population [50-60].
CONCLUSION
In a rather large population study, by exploring the importance of demographic and clinical features in the early postpartum period, our study showed a high incidence of PPD. Our results showed that women’s age and level of education could be directly related to PPD and could be included as risk factors. Further studies should be focused on younger women with a lower level of education which should have a closer follow-up during the early post-partum period to prevent adverse outcomes.
ACKNOWLEDGMENTS: None
CONFLICT OF INTEREST: None
FINANCIAL SUPPORT: None
ETHICS STATEMENT: The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee of the Ovidius University from Constanta, Romania (Registration No. 29726/31.05.2021).
References
- McNab S, Fisher J, Honikman S, Muvhu L, Levine R, Chorwe-Sungani G, et al. Comment: Silent burden no more: A global call to action to prioritize perinatal mental health. BMC Pregnancy Childbirth. 2022;22(1):308. doi:10.1186/s12884-022-04645-8
- Bach B, Sellbom M, Skjernov M, Simonsen E. ICD-11 and DSM-5 personality trait domains capture categorical personality disorders: Finding a common ground. Aust N Z J Psychiatry. 2018;52(5):425-34. doi:10.1177/0004867417727867
- Howard LM, Molyneaux E, Dennis CL, Rochat T, Stein A, Milgrom J. Nonpsychotic mental disorders in the perinatal period. Lancet. 2014;384(9956):1775-88.
- Saxton DL, Archer NP. The effect of postpartum depressive symptoms (PDS) on maternal health practices after childbirth, Texas pregnancy risk assessment monitoring system, 2012-2015. Matern Child Health J. 2022;26(3):537-44. doi:10.1007/s10995-021-03304-2
- Hanach N, Radwan H, Fakhry R, Dennis CL, Issa WB, Faris ME, et al. Prevalence and risk factors of postpartum depression among women living in the United Arab Emirates. Soc Psychiatry Psychiatr Epidemiol. 2023;58(3):395-407. doi:10.1007/s00127-022-02372-1
- Woldeyohannes D, Tekalegn Y, Sahiledengle B, Ermias D, Ejajo T, Mwanri L. Effect of postpartum depression on exclusive breast-feeding practices in sub-Saharan Africa countries: A systematic review and meta-analysis. BMC Pregnancy Childbirth. 2021;21(1):113. doi:10.1186/s12884-020-03535-1
- Terrone G, Bianciardi E, Fontana A, Pinci C, Castellani G, Sferra I, et al. Psychological characteristics of women with perinatal depression who require psychiatric support during pregnancy or postpartum: A cross-sectional study. Int J Environ Res Public Health. 2023;20(8):5508.
- Berger A, Schenk K, Ging A, Walther S, Cignacco E. Perinatal mental health care from the user and provider perspective: Protocol for a qualitative study in Switzerland. Reprod Health. 2020;17(1):26. doi:10.1186/s12978-020-0882-7
- Cox JL, Holden JM, Sagovsky R. Detection of postnatal depression. Development of the 10-item Edinburgh postnatal depression scale. Br J Psychiatry. 1987;150(6):782-6.
- Bradshaw H, Riddle JN, Salimgaraev R, Zhaunova L, Payne JL. Risk factors associated with postpartum depressive symptoms: A multinational study. J Affect Disord. 2022;301:345-51.
- Paddy A, Asamoah-Gyimah K, Nkyi A. Psychosocial determinants of postpartum depression and maternal well-being among postnatal women. Open J Psychiatry. 2021;11(3):138-59.
- Stewart D, Vigod SN. Postpartum depression: Pathophysiology, treatment, and emerging therapeutics. Ann Rev Med. 2019;70:183-96.
- Wang Y, Li B, Zhou Y, Wang Y, Han X, Zhang S, et al. Does endometriosis disturb mental health and quality of life? A systematic review and meta-analysis. Gynecol Obstet Invest. 2021;86(4):315-35.
- Han L, Zhang J, Yang J, Yang X, Bai H. Between personality traits and postpartum depression: The mediated role of maternal self-efficacy. Neuropsychiatr Dis Treat. 2022;18:597-609.
- Mercier RJ, Garrett J, Thorp J, Siega-Riz AM. Pregnancy intention and postpartum depression: Secondary data analysis from a prospective cohort. BJOG: An Int J Obstet Gynaecol. 2021;120(9):1116-22.
- Xie T, Fan X, Pang H, Zang T, Wu N, Liu J, et al. Association between gut microbiota and its functional metabolites with prenatal depression in women. Neurobiol Stress. 2023;28:100592. doi:10.1016/j.ynstr.2023.100592
- Huang W, Wu X, Yao Z, Gu Y, Lai X, Meng L, et al. Investigating the relationship between hepatitis B virus infection and postpartum depression in Chinese women: A retrospective cohort study. Front Public Health. 2023;11:1214151. doi:10.3389/fpubh.2023.1214151
- Dagklis T, Tsakiridis I, Chouliara F, Mamopoulos A, Rousso D, Athanasiadis A, et al. Antenatal depression among women hospitalized due to threatened preterm labour in a high-risk pregnancy unit in Greece. J Matern-Fetal Neonatal Med. 2018;31(7):919-25.
- Wisner KL, Sit DKY, McShea MC, Rizzo DM, Zoretich RA, Hughes CL, et al. On set timing, thoughts of self-harm, and diagnoses in postpartum women with screen-positive depression findings. JAMA Psychiatry. 2013;70(5):490-8.
- Zeng X, Yan X, Yang Y, Peng Z, Wei S, Chen J, et al. A correlation analysis on the postpartum anxiety disorder and influencing factors in puerperae with gestational diabetes mellitus. Front Endocrinol (Lausanne). 2023;14:1202884. doi:10.3389/fendo.2023.1202884
- Zubaran C, Schumacher M, Roxo MR, Foresti K. Screening tools for postpartum depression: Validity and cultural dimensions. Afr J Psychiatry. 2010;13(5):357-65.
- Sixty-fifth world health assembly. The global burden of mental disorders and the need for a comprehensive, coordinated response from health and social sectors at the country level. Available from: https://apps.who.int/gb/ebwha/pdf_files/WHA65/A65_R4-en.pdf (accessed July 21, 2023); 2012.
- McKee MD, Zayas LH, Jankowski KRB. Breastfeeding intention and practice in an urban minority population: relationship to maternal depressive symptoms and mother-infant closeness. J Reprod Infant Psychol. 2004;22(3):167-81.
- Xayyabouapha A, Sychareun V, Quyen BTT, Thikeo M, Durham J. Prevalence and risk factors associated with postpartum depressive symptoms among women in Vientiane Capital, Lao PDR. Front Public Health. 2022;10:791385.
- Barbadoro P, Cotichelli G, Chiatti C, Simonetti ML, Marigliano A, Di Stanislao F, et al. Socio-economic determinants and self-reported depressive symptoms during postpartum period. Women Health. 2012;52(4):352-68. doi:10.1080/03630242.2012.674090
- Vigod SN, Villegas L, Dennis CL, Ross LE. Prevalence and risk factors for postpartum depression among women with preterm and low-birthweight infants: A systematic review. BJOG: An Int J Obstet Gynaecol. 2010;117(5):540-50. doi:10.1111/j.1471-0528.2009.02493.x
- Solis M, Valverde-Barea M, Gutiérrez-Rojas L, Romera I, Cruz-Bailén S, Jiménez-Fernández S. Suicidal risk and depression in pregnant women in times of pandemic. Matern Child Health J. 2023;27(9):1540-7. doi:10.1007/s10995-023-03688-3
- Rai S, Pathak A, Sharma I. Postpartum psychiatric disorders: Early diagnosis and management. Indian J Psychiatry. 2015;57(Suppl 2):S216-21.
- VanderKruik R, Barreix M, Chou D, Allen T, Say L, Cohen LS. Maternal morbidity working group. the global prevalence of postpartum psychosis: A systematic review. BMC Psychiatry. 2017;17(1):272.
- Roy-Byrne P. Postpartum blues and unipolar depression: Epidemiology, clinical features, assessment, and diagnosis. Up-to-date, Post, TW (Ed), Uptodate, Waltham, MA; 2016.
- Johnson J, Hope L, Jones L, Bradley E. A mixed methods study to understand perinatal mental healthcare referral decisions among midwives and health visitors in the UK. Front Psychiatry. 2023;14:1056987. doi:10.3389/fpsyt.2023.1056987
- Shorey S, Chee CYI, Ng ED, Chan YH, Tam WWS, Chong YS. Prevalence and incidence of postpartum depression among healthy mothers: A systematic review and meta-analysis. J Psychiatr Res. 2018;104:235-48.
- Saldanha D, Rathi N, Bal H, Chaudhari B. Incidence and evaluation of factors contributing towards postpartum depression. Med J Dr. D.Y. Patil Univ. 2014;7(3):309-16.
- Ozturan DD, Gulucu S, Ozsoy F. The role of early maladaptive schemas in postpartum depression. Hindawi. Perspect Psychiatr Care. 2023;2023.
- Eurostat, an official website of the European Union 2021. Available from: https://ec.europa.eu/eurostat/web/products-eurostat-news/-/ddn-20210224-1 (accessed on 27 July 2023); 2021.
- Anding J, Röhrle B, Grieshop M, Schücking B, Christiansen H. Early detection of postpartum depressive symptoms in mothers and fathers and its relation to midwives’ evaluation and service provision: A community-based study. Front Pediatr. 2015;3:62.
- Dubey A, Chatterjee K, Chauhan VS, Sharma R, Dangi A, Adhvaryu A. Risk factors of postpartum depression. Ind Psychiatry J. 2021;30(Suppl 1):S127-31.
- Zarghami M, Abdollahi F, Lye M. A comparison of the prevalence and related risk factors for post-partum depression in urban and rural areas. Iran J Psychiatry Behav Sci. 2019;13(2):e62558.
- Vigod SN, Tarasoff LA, Bryja B, Dennis CL, Yudin MH, Ross LE. Relation between place of residence and postpartum depression. CMAJ. 2013;185(13):1129-35.
- Delcea C, Bululoi AS, Gyorgy M, Rad D. Psychological distress prediction based on maladaptive cognitive schemas and anxiety with random forest regression algorithm. Pharmacophore. 2023;14(5):62-9. doi:10.51847/ukrb1pafyv
- Doraiswamy S, Jithesh A, Chaabane S, Abraham A, Chaabna K, Cheema S. Perinatal mental illness in the middle east and north Africa region-A systematic overview. Int J Environ Res Public Health. 2020;17(15):5487. doi:10.3390/ijerph17155487
- Gyorgy M, Delcea C, Enache A. The role of maladaptive cognitive schemas in decision making in offenders charged with murder. Roman J Leg Med. 2023;31(14):92-6. doi:10.4323/rjlm.2023.92
- Gherman C, Enache A, Delcea C, Siserman C. An observational study on the parameters influencing the duration of forensic medicine expert reports in assessment of inmates’ health status in view of sentence interruption on medical grounds - conducted at the Cluj-Napoca legal Medicine Institute between 2014 and 2018. Roman J Leg Med. 2019;27(2):156-62. doi:10.4323/rjlm.2019.156
- Mulugeta Y, Mohammed AA, Ibrahim IM, Getachew G, Ahmed KY. Postpartum depression and associated factors in Afar Region, northeast Ethiopia. Heliyon. 2023;9(9):e19914. doi:10.1016/j.heliyon.2023.e19914
- Zejnullahu VA, Ukella-Lleshi D, Zejnullahu VA, Miftari E, Govori V. Prevalence of postpartum depression at the clinic for obstetrics and gynecology in Kosovo teaching hospital: Demographic, obstetric and psychosocial risk factors. Eur J Obstet Gynecol Reprod Biol. 2021;256:215-20.
- Giannandrea SAM, Cerulli C, Anson E, Chaudron LH. Increased risk for postpartum psychiatric disorders among women with past pregnancy loss. J Women’s Health (Larchmt). 2013;22(9):760-8.
- Field T. Postnatal anxiety prevalence, predictors and effects on development: A narrative review. Infant Behav Dev. 2018;51:24-32. doi:10.1016/j.infbeh.2018.02.005
- Citu C, Gorun F, Motoc A, Sas I, Burlea B, Citu IM, et al. Prevalence and risk factors of postpartum depression in Romanian women during two periods of COVID-19 pandemic. J Clin Med. 2022;11(6):1628.
- Matei A, Dimitriu MCT, Cirstoveanu CG, Socea B, Ionescu CA. Assessment of postpartum depression in adolescents who delivered during COVID-19 social restrictions: The experience of a tertiary hospital from Bucharest, Romania. Healthcare (Basel). 2021;9(7):807.
- Siserman C, Delcea C, Matei HV, Vică ML. Major affective distress in testing forensic paternity. Rom J Leg Med. 2019;27(3):292-6.
- Delcea C, Siserman C. Validation and standardization of the questionnaire for evaluation of paraphilic disorders. Rom J Leg Med. 2020;28(1):14-20.
- Siserman C, Giredea C, Delcea C. The comorbidity of paraphilic disorders and rape in individuals incarcerated for sexual offences. Rom J Leg Med. 2020;28(3):278-82. doi:10.4323/rjlm.2020.278
- Gherman C, Enache A, Delcea C. The multi-factorial determinism of forensic expertise regarding sentence interruption on medical grounds and decision. J Forensic Leg Med. 2019;61:45-55.
- Rus MR, Matei ML, Sandu C, Delcea C, Siserman S. Emotional distress and coping strategies of health care workers during Covid-19 pandemic. Rom J Leg Med. 2020;28(4):442-50. doi:10.4323/rjlm.2020.442
- Banariu GM, Delcea C, Tica I, Rus M, Neagoe G, Onuc S, et al. Covid-19 a potent cocktail with associated mental problems: The psychosomatic effects in pregnant women - An interdisciplinary approach. Rom J Leg Med. 2022;30(4):325-30. doi:10.4323/rjlm.2022.325
- Delcea C, Siserman CV. The emotional impact of COVID-19 on forensic staff. Rom J Leg Med. 2021;29(1):142-6. doi:10.4323/rjlm.2021.142
- Delcea C, Rad D, Toderici OF, Bululoi AS. Posttraumatic growth, maladaptive cognitive schemas and psychological distress in individuals involved in road traffic accidents—A conservation of resources theory perspective. Healthcare. 2023;11(22):2959. doi:10.3390/healthcare11222959
- Delcea C, Rad D, Gyorgy M, Runcan R, Breaz A, Gavrilă-Ardelean M, et al. A network analysis approach to Romanian resilience - Coping mechanisms in the Covid-19 era. Pharmacophore. 2023;14(4):57-63. doi:10.51847/OdzZJceF6O
- Nicoară ND, Marian P, Petriș AO, Delcea C, Manole F. A review of the role of cognitive-behavioral therapy on anxiety disorders of children and adolescents. Pharmacophore. 2023;14(4):35-9. doi:10.51847/lKULo5pB1T
- Voiță-Mekereș F, Voiță GF, Pogan MD, Delcea C, Manole F, Mekereș GM, et al. Clinical considerations of dental longevity from the lateral area. Pharmacophore. 2023;14(3):100-6. doi:10.51847/7bv11U51PZ
