Archive \ Volume.15 2024 Issue 2
Drug-Drug Interaction Between Fluconazole and Vancomycin: A Case Report
, ,Abstract
We present the case of a probable pharmacokinetic drug-drug interaction (DDI) between fluconazole (FLU) and vancomycin (VCM), in a patient who underwent hepatobiliary surgery, and biliary drainage, and was under treatment with vancomycin, meropenem, and fluconazole, due to infectious pathology. Changes in the kinetic process of VCM and FLU has not been fully elucidated. Therefore, understanding the changes in renal transporters involved in the renal excretion pathway of VCM and FLU (e.g. multidrug resistance-associated proteins, organic cation transporters, P-glycoprotein) is beneficial in predicting better drug disposition and optimize optimizing dosing. Inhibition of the aforementioned transporters is a common mechanism underlying DDIs. After pharmacokinetic monitoring of VCM treatment, the trough concentration values and the half-life of VCM showed an abnormally unexpected increase when VCM was used in combination with FLU, compared to data obtained when vancomycin was used without fluconazole. Said changes, of the pharmacokinetic parameters studied, would support a DDI between FLU and VCM. Because of this, special caution is required whenever VCM is co-administered with fluconazole, and close monitoring of VCM trough concentrations is recommended to minimize the risk of toxicity.
How to cite:
Download Citation
INTRODUCTION
Vancomycin (VCM) is a glycopeptide antibiotic used to treat a number of bacterial infections. This treatment is recommended intravenously for complicated infections of the skin, bloodstream, bones, and joints, as well as endocarditis and meningitis caused by methicillin-resistant Staphylococcus aureus [1] it has long been the gold standard for suspected or known infections caused by this pathogen [2].
Monitoring has made it possible to establish therapeutic ranges (10-20 mg/L) that prevent toxicity due to supratherapeutic levels. However, their joint use with drugs, especially nephrotoxic drugs (e.g., gentamicin, amikacin, tobramycin, colistin), and pharmacokinetic drug-drug interactions (DDI), alter their elimination and increase the risk of toxicity (e.g., nephro and ototoxicity) [3].
In this case report, we present the first documented case of a probable pharmacokinetic DDI between vancomycin and fluconazole (FLU).
Case Presentation
A 78-year-old patient, with no known drug allergies and a medical history of dyslipidemia, microhematuria (in 2015), and hydatid cyst (in 2016), on atorvastatin (10 mg/24h) as the only common medication, underwent surgery (01/13/2023) due to purulent peritonitis secondary to duodenal perforation. The subsequent evolution was favorable, showing a progressive decrease in bile output through the drains, which allowed Kehr’s tube to be kept closed for 24 hours and, finally, the closure of the primary drainage, through laparotomy under general anesthesia (02/02/2023) with the suture of the gastroenteric and bile duct anastomosis.
Empirical antibiotic therapy, with Meropenem + Anidulafungin + Tigecycline, was instituted after surgery (01/13/2023), de-escalating with the microbiological results to fluconazole, stopping tigecycline and maintaining meropenem. Because of the unfavorable evolution of the biliary fistula, drainage cultures were extracted and empirical broad-spectrum antibiotic therapy was restarted to treat a sepsis of probable biliary origin, on February 2, 2023 (day 0), maintaining meropenem (1g/8h) added to vancomycin (EV 1g/12h) (Table 1, Figure 1). This was taken together with subcutaneous enoxaparin (40 mg/24h), metamizole (EV 2g/8h), and omeprazole (EV 40 mg/12h).
|
Table 1. Evolution of half-life and vancomycin trough concentration values, and creatinine according to vancomycin dosage regimen and day of treatment (day 0 corresponding to 02/03/2023). |
||||
|
Vancomycin Treatment |
||||
|
Day |
Dosage regimen |
Creatinin (mg/dl) |
Vancomycin trough concentration (mcg/ml) |
Half-life (h-1) |
|
1 |
1g/12h |
0.33 |
13.4 |
8.2 |
|
3 |
1g/12h |
0.33 |
13.1 |
8.1 |
|
5 |
1g/12h |
0.47 |
24.6 |
12.8 |
|
8 |
0.75g/12h |
0.37 |
23.9 |
14.6 |
|
10 |
0.5g/12h |
0.46 |
23.3 |
19.7 |
|
12 |
0.75g/12h |
0.4 |
24 |
18.4 |
|
14 |
1g/12h |
0.51 |
25.7 |
15.8 |
|
17 |
1g/24h |
0.49 |
9.1 |
13.7 |
|
19 |
0.75g/12h |
0.34 |
12.6 |
9.7 |
 |
|
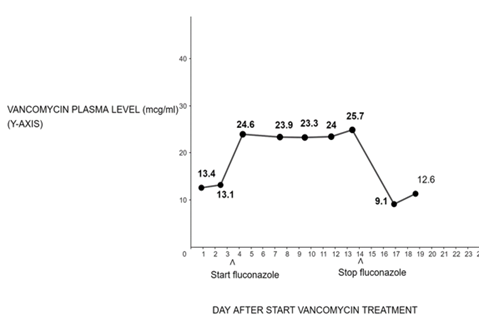
Figure 1. Trough concentration values vs day after start of vancomycin treatment. The start date of vancomycin is set to day 0 and the combination of fluconazole plus vancomycin starts on day 4 and ends on day 15. The antibiotics used during the course of treatment included meropenem, vancomycin, and vancomycin plus fluconazole. |
After microbiological results, treatment with fluconazole (EV 400 mg single dose on day 4, followed by 200/24h from day 5 to 15), in addition to meropenem (1g/8h from day 1 to 21) and vancomycin (EV dose according to levels every 12-24h from day 1 to 21) (Table 1, Figure 1) was maintained and stopped after 21 days, due to the patient's good progress. This was taken together with dexketoprofen (PO 25 mg/8h, if necessary), enoxaparin (SC 40 mg/24h, throughout the hospitalization), lorazepam (PO 1 mg/24h, if necessary), omeprazole (EV 40 mg/24h followed by omeprazole PO 20 mg/24h, throughout the hospitalization) and paracetamol (EV 1g/8h followed by paracetamol PO 1g/24h, if necessary, throughout the hospitalization).
Subsequent evolution was favorable, with the patient being afebrile and in good general condition at the time of discharge, tolerating an oral diet, with normal abdominal examination, restored transit (daily bowel movements), and laboratory tests in the normal range. Finally, on February 19, 2023, the patient was transferred to the surgical ward, where the evolution was slowly favorable until February 24.
After pharmacokinetic monitoring of vancomycin (VCM) treatment, the trough plasma concentration values and the half-life of VCM showed an abnormally unexpected increase when VCM was used in combination with fluconazole (FLU) (days 4 to 15), compared to data obtained when VCM was used without FLU (day 1 to 3 and 15 to 19). Indeed, a gradual increase in the half-life and plasma level of VCM was found, reaching a maximum value to subsequently decrease to values well above normal, with increases of up to double its initial value, compared to the previous period without treatment with FLU. An increase that, when comparing the pharmacological treatment in both periods, and in the absence of pharmacokinetic, pharmacodynamic, and/or pathophysiological factors, has been attributed to probable DDI between FLU-VCM, according to a score of 6 on the Drug Interaction Probability Scale (DIPS) (6 = probable) [4].
To calculate pharmacokinetic parameters, we used a VCM calculator that uses population pharmacokinetic estimates, Bayesian models, and the Sawchuk-Zaske method to calculate a VCM dosing regimen for an adult patient. VCM regimens can be calculated using a VCM level. The half-life was used as a pharmacokinetic parameter to follow the evolution of the interaction, with the aim of better visualization, since the plasmatic levels of the drug vary with the dose adjustments.
RESULTS AND DISCUSSION
Three mechanisms have been described for the tubular secretion system of renal excretion of drugs (e.g., VCM), one mediated by organic cation transporters, another by organic anions, and a third mediated by P-glycoprotein (P-gp) (for example cephalosporins, vancomycin). Such drug transport systems within tubular cells play an important role in the development of DDI [5]. Therefore, some lipophilic anti-infective agents [e.g., fluconazole, inhibit P-gp [6] and, additionally, multidrug resistance-associated proteins (MRPs) and organic anion transporters (OATs)] are involved in its distribution [7]; furthermore, hydrophilic anti-infective agents (e.g., VCM), are often cleared unchanged by renal glomerular filtration and tubular secretion, and may compete with other drugs (e.g., FLU) for the use of transporters for their excretion [2].
In fact, said renal excretion, therefore, would be mediated by specific transporters in the basolateral and apical membranes of the proximal tubule epithelium [8], such as OATs, especially OAT1 and OAT3 [9] (organic cation transporters, OCTs) [10], especially OCT2, and P-gp, among others.
However, its relationship with changes in the kinetic process of VCM has not been fully elucidated. Therefore, understanding the changes in renal transporters involved in the renal excretion pathway is beneficial in predicting better drug disposition and optimizing dosing. Inhibition of the aforementioned transporters is a common mechanism underlying DDIs.
FLU and VCM do not inhibit any transporter beyond 60%, however, sufficient to elicit clinically relevant DDI [7]. Some studies also suggest that azole antifungals may interact with P-gp and that this would affect both disposition and exposure to azole antifungal treatments and partially explain the observed clinical drug interactions [6].
CONCLUSION
In short, we present the case of a possible pharmacokinetic DDI between FLU and VCM, in a patient under treatment with vancomycin, meropenem, and fluconazole, due to hepatobiliary surgery and biliary drainage infected by Klebsiella pneumoniae and Enterococcus faecium. The patient had stable renal function without significant changes in the doses of his other medications during treatment with VCM. After pharmacokinetic monitoring of VCM treatment, the trough concentration values and the half-life of VCM showed an abnormally unexpected increase, when VCM was used in combination with FLU, compared to data obtained when VCM was used without FLU, through competitive inhibition of transporters involved in the tubular secretion mechanism of VCM as a possible cause.
These changes in the pharmacokinetic parameters studied would support a DDI between FLU and VCM. Therefore, special caution is required whenever VCM is co-administered with FLU, and close monitoring of VCM trough concentrations is recommended to minimize the risk of nephrotoxicity.
ACKNOWLEDGMENTS: None
CONFLICT OF INTEREST: None
FINANCIAL SUPPORT: None
ETHICS STATEMENT: Ethical approval is not required for this study following the local IRB. The patient’s informed consent was obtained during the assessment visits.
References
- Liu C, Bayer A, Cosgrove SE, Daum RS, Fridkin SK, Gorwitz RJ, et al. Clinical practice guidelines by the Infectious Diseases Society of America for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children: executive summary. Clin Infect Dis. 2011;52(3):285-92.
- Klevens RM, Edwards JR, Tenover FC, McDonald LC, Horan T, Gaynes R. Changes in the epidemiology of methicillin-resistant Staphylococcus aureus in intensive care units in US hospitals, 1992–2003. Clin Infect Dis. 2006;42(3):389-91.
- Technical sheet vancomycin Pfizer 500 mg powder for concentrate for solution for infusion EFG. Available from: https://cima.aemps.es/cima/dochtml/ft/73784/FT_73784.html
- Horn JR, Hansten PD, Chan LN. Proposal for a new tool to evaluate drug interaction cases. Ann Pharmacother. 2007;41(4):674-80.
- Fanos V, Cataldi L. Renal transport of antibiotics and nephrotoxicity: A review. J Chemother. 2001;13(5):461-72.
- Pea F, Furlanut M. Pharmacokinetic aspects of treating infections in the intensive care unit: Focus on drug interactions. Clin Pharmacokinet. 2001;40(11):833-68.
- Wang W, Zheng N, Zhang J, Huang X, Yu S. Effect of efflux transporter inhibition on the distribution of fluconazole in the rat brain. Neurochem Res. 2017;42(8):2274-81.
- Guo X, Meng Q, Liu Q, Wang C, Sun H, Peng J, et al. JBP485 improves gentamicin-induced acute renal failure by regulating the expression and function of Oat1 and Oat3 in rats. Toxicol Appl Pharmacol. 2013;271(2):285-95.
- Liu T, Meng Q, Wang C, Liu Q, Guo X, Sun H, et al. Changes in expression of renal Oat1, Oat3, and Mrp2 in cisplatin-induced acute renal failure after treatment of JBP485 in rats. Toxicol Appl Pharmacol. 2012;264 (3):423-30.
- Fransson M, Helldén A, Östholm Balkhed Å, Nezirević Dernroth D, Ha M, Haglund M, et al. Case report: Subtherapeutic vancomycin and meropenem concentrations due to augmented renal clearance in a patient with intracranial infection caused by streptococcus intermedius. Front Pharmacol. 2021;12:728075.
